This is the section of the Mental Health Act (MHA) review final report reflecting the views and input of service users. The MHA review involved, consulted and sought input from service users on an unprecedented scale and whatever happens to the final recommendations the feedback, perspecive and findings from service users should be widely shared not buried on some shelf at the department of health. Also people can link to it when they are getting #notallprofs lines from professionals or ‘that’s just your experience’… Well no, according to the MHA review it isn’t:-
SERVICE USER EXPERIENCE Pages 53-58 MHA Review
Service users have been at the heart of this Review, and we want to make sure their voices are clearly heard in this report. This section pulls together some key themes from the patient experiences that have been shared with us through our service users and carers survey, individual and group submissions, focus groups, engagement events and service user and carer group. We would like to thank those who contributed to debates, shared views and opinions and often revisited difficult or traumatic periods of their lives in order to help us. We should also like to thank any who facilitated feedback or made their own contributions as relatives, carers and friends. And in particular, we would like to thank our Service User and Carer Group which has been invaluable in helping us to shape our recommendations. Patients and carers have told us it is vital that their experiences, and their knowledge of what works best for them, are recognised and acted on, by this Review.
Overall, we have been disturbed and saddened by what we have heard from patients. Only 30% of respondents to our survey of service users and carers felt that they had been treated with dignity and respect, and whilst we accept that surveys like ours can sometimes have a bias towards recording experiences at the extreme ends of the positive/negative scale, this is clearly very worrying. Too many people are detained in wards that are far below the standard anyone would want for themselves or their loved ones. We are also aware that there is sometimes a disconnect between how staff perceive the care they give, and how it is experienced by patients. We agree. Too many have found that when they have previously voiced reasonable concerns or complaints, or spoken of the trauma detention and treatment has caused them, they have been ignored, or their accounts have been dismissed as being due to symptoms of disorder (an example of epistemic injustice, see box).
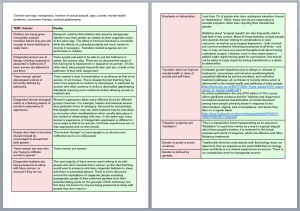
Epistemic injustice occurs when a person’s capacity as a person with knowledge is wrongfully denied. It is a phrase that some service users feel represents elements of their experiences during the detention process. Epistemic injustice could be when a person’s credibility is challenged for no good reason and their testimony is not believed. An example might be when a person’s treatment preferences are dismissed because the individual’s mental health diagnosis suggests that they are unable to think clearly or rationally about their options.
Some patients have reported neglect, both of physical and psychological health, and the experience of receiving impersonal care, leaving them feeling processed rather than cared for:
- Many patients report being disparaged, disbelieved or ignored and have been subject to judgemental and paternalistic behaviour from those caring for them.
- Some patients report coercive mistreatment such as the use of access to leave, or contact with families, as levers in order to achieve compliance, for example making ward leave or access to the telephone dependent on behaviour. Forced compliance can lead to institutionalisation which can delay recovery.
- Hierarchical ward structures can mirror the negative experiences patients have had with other authority figures.
- Lack of privacy is a problem – about 1000 inpatient beds are still in multiple bedded rooms. People face arbitrarily imposed restrictions such as being shut out of bedrooms during the daytime, or locked in bedrooms at night. This can increase levels of mental ill-health.
- Many find it hard to retain links to their social networks and communities whilst detained and many lose contact with family and friends, as well as losing home, employment, or access to education. This can lead to patients being much worse off than before they were detained, for example being unable to work, homeless38 or worse.
- Parents and carers of children, and those with learning disabilities or autism, told us that professionals do not always take the time to understand how best to communicate with a person with a learning disability, autism or both to try and understand what is causing their distress, or have the necessary skills to do so. We also heard that their attempts to share information and to remain supportive and involved when someone is detained have led them to be ignored or excluded because they are seen as ‘too dominant’, ‘overbearing’ or ‘over-involved’.
- We have heard repeatedly of the distressing and unacceptable experiences from people from ethnic minority communities and in particular black African Caribbean men. Fear of what may happen if you are detained, how long you may be in hospital and even if you will get out are all widespread in ethnic minority communities. Addressing the issues facing this group of people is a central priority for the Review.
- Patients detained under the criminal justice system suffer from even longer delays to access the care they need.“A new patient kept ringing the police. They told us that if she didn’t stop then they would take the phone away. It was the only way we could talk to our families.” 39 – Service User“In my Trust they have adopted the tactic of explicitly framing complaint- making by patients against staff and services as an indication that the patient is a risk to others, and formally recording this ‘risk’ in the risk assessments they use to make decisions regarding leave and discharge, etc.” Service user.
Patients also reported harassment and abuse on inpatient wards, both physical and sexual. A CQC review41 reported 1,120 sexual safety reports from Apr-June 2017, of which more than a third of the incidents (457) could be categorised as sexual assault or sexual harassment of patients or staff. Data collection is inconsistent on this, and could be improved as it is for restraint. From the date that is available we know that restraint continues to be a routine occurrence on many wards, affecting disproportionately those from ethnic minority populations, women and girls. Restraint, and particularly pain-based restraint and prone restraint, can be frightening and life threatening. Not surprisingly, sexual assaults and restraint can lead to lasting trauma for those affected.
Ward physical environments have become increasingly cold and unwelcoming with an emphasis on physical safety. A few people have even told us that the way they are treated by staff, the levels of threat and violence, the physical environment and the sound levels make hospitals seem little different to prison.
We are acutely aware that this will be an uncomfortable read. It will be difficult for some of those who provide care, or those reading this report, to comprehend and accept the poor experiences that many patients suffer. But it is essential that they find the courage to acknowledge what patients are saying has been their experience rather than what their care providers believe they provide, if care and treatment are to improve. Many of the issues we cover here have been highlighted repeatedly in CQC reports and by service users and their families. Other problems have slipped below the radar, in some cases because of low expectations of what constitutes good care, and in others because of poor quality assurance of the care provided on wards. The CQC inspection criteria should also be strengthened, for example to have a greater focus on therapeutic environments and person centred care that meets the needs of people with a range of equality characteristics. Day-to-day reporting of incidents is inconsistent and numerous and complex complaints processes prevent patients and relatives from obtaining redress. Those that do complain have told us that care can be negatively affected. All of this has allowed everyone, from local ward staff to national system leaders to overlook or even normalise poor practice.
We are also aware of the huge dedication and compassion of thousands of staff across the NHS, Local Authorities and other agencies, and how services and staff suffer when they are over-stretched, feel overwhelmed and unsupported. High bed occupancy, rapid turnover of patients, higher levels of detention, regulatory pressures, and increased administrative work and inefficient processes can all reduce time spent therapeutically with patients and reduce job satisfaction for staff. Lack of staff and high levels of temporary or ill-equipped staff contribute to wards with high levels of coercion and conflict42. Increasing vacancies (14.3% for MH nursing43, 9% for consultant posts44, 2017) and high turnover suggest the current culture and environment do not support either staff or patients and that this is becoming normalised. Improving ward culture would improve support for staff and help potential problems to be addressed before they escalate. In addition, pressures upon community NHS and social work services can lead to problems in appropriately discharging people.
Solutions to these problems must be multifaceted, addressing the needs of patients and considering how best to encourage and maintain wards that are therapeutic and respect patients’ rights. The Convention on the Rights of Persons with Disabilities (CRPD) 45requires that no decisions about disabled persons should take place without them, so those with relevant lived experience should be involved in decision making across the system, including co-design and production with patients at ward level. Patients should be treated in a way that respects them in the context of their own lives, recognises their strengths, needs, values and experiences and provides equality of outcome regardless of any disabilities or protected characteristics. It is not enough to merely ask that people detained under the Act are listened too, nor can we achieve our goals, of fair treatment for all, if detained patients continue to have so little say in their care and treatment. Many of the legal and regulatory changes recommended in this Review are essential to driving culture change, to ensuring shared decision making becomes routine practice, and that patients’ own expertise is acknowledged and valued.
“ Being sectioned was one of the most traumatic experiences of my life. Sadly, as a result of being sectioned I developed PTSD as the direct result of the way I was treated ” – Service user
“ I did not view the act of sectioning in my case as something that should be avoided, if you are physically exceptionally unwell you are placed in intensive care – the same arrangement applies to your mental health when in crisis ” Service user
Recovery In The Bin (RITB) is covered by a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) License