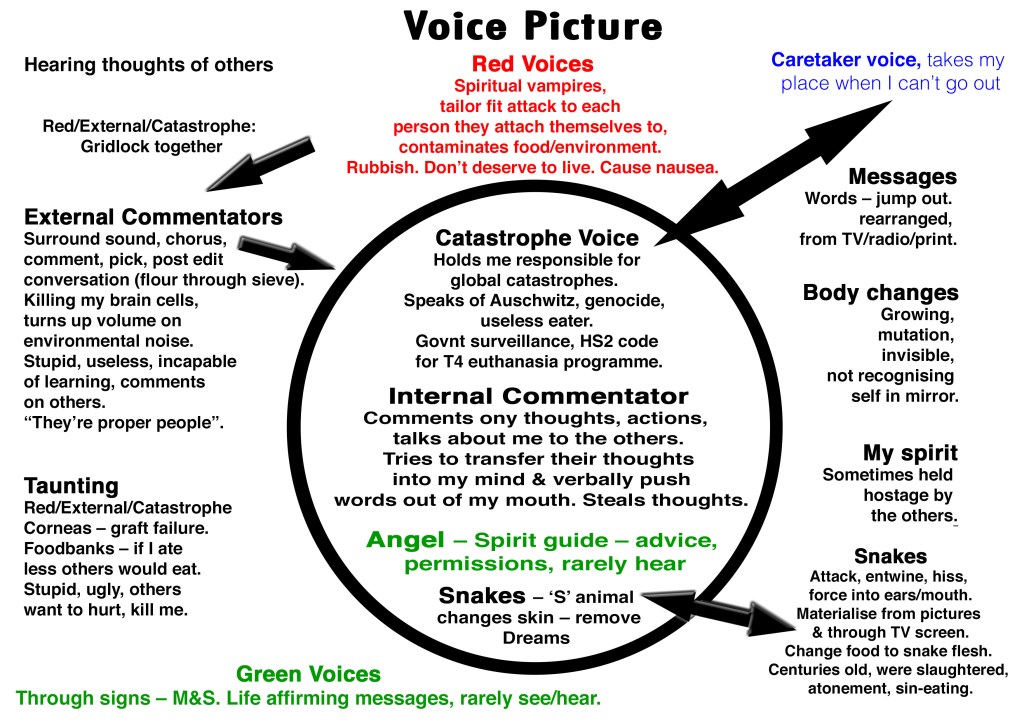
I am a voice hearer, I developed a form of testimony of my voices, something that I could share with others and do with other voice hearers.
A simple template that could be used by voice hearers, or with their friends, family, peers, within hearing voices groups.
For a voice hearer to share with a mental health professional as a starting point for conversation about voices, or something initiated within that support.
The important part of this process is that the voice hearer is leading it. This isn’t about diagnosis, formulation or treatment, it is a simple method of testimony of experience, entirely in the voice hearers own words.
How to do your Voice Picture
Take a piece a paper, A4 or larger and draw a circle in the middle, this represents your head.
Voices can often be heard inside and outside of our heads, or with external voices (or thoughts or sounds) crossing over to inside our heads, and vice versa.
Some of us also see our voices/entities, or have tactile voices we feel, or someones all three, hearing, feeling and seeing.
Identify your voices
Give your voices/sounds, be they individual or groups names. Identify numbers of them, gender, colours, what they say, how they say it.
You can write as much or as little as you like, a single word, or several sentences.
Voice Recreation
This is producing anything from a small snapshot of your voices to however sophisticated you want to get!
You could use your own voice, that of friends, other voice hearers, create sounds, use everyday objects for creating sounds.
Then record it on anything from your mobile phone to using sound software.
Your voice picture and soundscape are your personal testimony for you to do whatever you wish with, whether it’s a personal conversation with yourself and your voices, or something you share with others to say “these are my voices”.
If you met me in everyday life, you probably wouldn’t guess much about my past.
I work. I have hobbies. I have friends. I have interests, hopes, dreams, and the usual regrets people carry through life. On the surface, I’m just another person getting on with things.
What you can’t see is what I’ve survived.
I’m a survivor of complex childhood trauma, including child sexual abuse. I’m also autistic and live with bipolar disorder and complex PTSD. These things shape my life every day, even when they aren’t visible.
Like many people with trauma histories, I’ve spent years trying to rebuild a life while navigating systems that often struggle to understand people like me. Again and again I’ve encountered the same barriers: a lack of awareness about autism in women, a lack of understanding about trauma, and mental health services that too often fail the people who rely on them most.
The hardest part is the bitter irony at the centre of all this.
The people who abused me never faced consequences.
Yet somehow I have ended up the one being labelled as the problem.
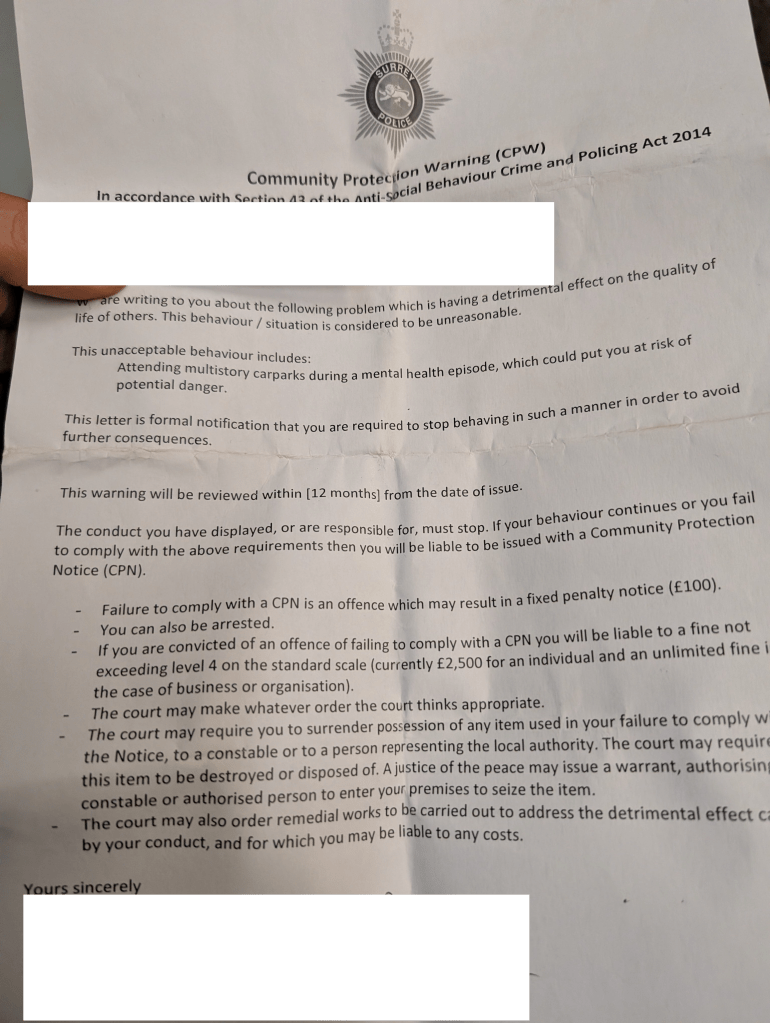
After a suicide attempt, I received a Community Protection Warning from the police.
It’s difficult to describe what that feels like. When someone reaches the point of attempting to end their life, they are already at the edge of what they can carry. In that moment, the response you hope for from public services is care, protection, and understanding.
Instead, I was treated as though my distress itself was the issue that needed controlling.
The experience left me feeling as though surviving trauma had somehow become something I could be punished for.
Conversations I’ve had since suggests the current use of Community Protection Warnings may be a replacement for earlier “demand management” initiatives such as the High Intensity Network and Serenity Integrated Mentoring (SIM) model. Those schemes were widely criticised for criminalising people in mental health crisis.
What troubled me even more was the reasoning described in the Professional Standards Department response.
The justification for the action appeared to centre on reducing police demand and resources, rather than safeguarding someone in crisis.
A clinician involved in my care later reported a phone call with the officer responsible for the warning. During that conversation, the officer was told that the measure had caused harm and increased my risk of suicide. According to the clinician’s account, the officer indicated that this outcome was considered acceptable because it reduced police demand and was part of a wider approach rather than a decision specific to me.
Reading that was devastating.
It suggested that the harm caused wasn’t an unintended consequence. It was something that had effectively been weighed against resource pressures — and deemed acceptable.
Living with trauma and mental illness can sometimes feel like walking through the world with invisible injuries. You learn to keep it invisible. You build a life around them as best you can.
I understand more than most the reality of the funding pressures facing police. Pressures greater than NHS & social care but with less public awareness.
But being labelled now as the problem rather than a person needing help, or not even being seen as a person at all has hurt.
No one in suicidal crisis should face the threat of being criminalised for surviving.
And no system designed to protect the public should knowingly accept the risk that its actions might push someone closer to the edge
The full list of The RITAs Awards for Excellence in Awfulness 2025!
Patronising Interventions Award sponsored by having a cup of tea in a warm bath CIC (we’re Disability Confident™): The Decider life skills program for those for whom DBT has been deemed too expensive.
Bad Samaritan Award: The Samaritans (for rationing calltime)
Charity of the Year award for services to sponsored marathons: MIND
Professional Tosser Award (Joint): Jonathon Shedler and Mark Ruffalo (not the actor) For their verbal diarrhoea on X/Twitter
Marie Antoinette Award for Obliviousness: Prof Appleby fails to respond to survivors and ignores deaths caused by government policies including DWP and removal of Trans healthcare.
Worst description of survivors by professionals Award: “Sick role”
We are so rebellious that conservatives agree with us and we have book deals, and appear on TV: The Criticals – The nickname for professionals viewed as radical/critical thinking about MH services and disciplines yet aren’t revolutionary but are just seeking to replace one hierarchy with theirs.
Lifetime Achievement for Total Bollocks Award: Peter Tyrer – For his endless judgemental and stigmatising promotion of “Personality Disorder”. Runner up: Rachel Perkins
The Award Award, an award for the best award that health professionals award to each other at self congratulatory conferences. Sponsored by Ostrich Narcissus Private Equity Fund: BIGSPD – the annual party for personality disorder professionals to congratulate themselves.
Most extractive and exploitative false co-production award, sponsored by NHS England: Tim Kendall, for SIM
Worst Trust of the YearWinner: Norfolk and Suffolk NHS Foundation Trust (NSFT)
Nominated:
Cambridgeshire and Peterborough NHS Foundation Trust (CPFT)
Essex Partnership University NHS Foundation Trust (EPUT)
Greater Manchester Mental Health NHS Foundation Trust (GMMH)
Kent and Medway NHS and Social Care Partnership Trust (KMPT)
Lancashire and South Cumbria NHS Foundation Trust (LSCFT)
Norfolk and Suffolk NHS Foundation Trust (NSFT)
Surrey and Borders Partnership NHS Foundation Trust (SABP)
Tees, Esk and Wear Valleys NHS Foundation Trust (TEWV)
The Chocolate fireguard achievement in creative report writing award: Care Quality Commission CQC
Worst thing said to you by a health professional, Award sponsored by ‘its your choice, you have capacity to kill yourself’ (Joint):
“You do know that you have a Black gene that is causing you to be mentally ill”
“Your brain lacks the foundations of an ordinary building which is why you should take Sodium Valproate”
“Katy has a different kind of brain ”
“The thing about Sophie is, there’s nothing you can do to help her.”
“well you’re quite the prolific self harmer anyway. we’ve already decided you don’t need a bed, we just need to tick you off” (said to me as soon as they met me, before they even said hello).
“I ain’t going to coroner’s court for you & neither will your private therapist, the trust, or the ambulance service. You have capacity”. Then she (NHS rapid response service) hung up the phone on me. This was seconds after a suicide attempt when I was home alone.
“You can’t have autism, you don’t like trains”, said by an NHS psychiatrist medical director who had “worked with autistic people for many years”. (later diagnosed with autism).
“Nurse telling me to try losing weight with keto to cure anorexia has to be up there right? Apparently I’d lose ten kilos a month if I just ate as much meat as possible and nothing else. Impressive double whammy of ‘not how to help an anorexic’ and ‘not physiologically possible’.”
Refused help because you won’t meet services “recovery targets”
Award Goes to ‘The unknown professional’ for all these things that are said. You know who you are!
Worst Broadcaster: Channel 4, Fraser Nelson (Dispatches: Inside Britain’s £48 Billion Benefits Scandal). This was journalistic malpractice by Dispatches, Fraser Nelson has a well documented bias against social security and advocates for far right positions (noticeably he edited The Spectator, a magazine that has posted defences of Nazis -who under Aktion T4 exterminated 250,000 disabled people as a precursor to the Holocaust), this cherry picked meritless hit piece is beneath acceptable standards. The real story is the thousands of deaths caused by the DWP. deathsbywelfare.org
Most repulsive think tank: Centre for Social Justice
Political gaslighter of the Year Award: The government front bench & the Westminster media lobby.
You can’t call someone a liar in parliament, but we’re not in parliament, so LIAR! Award: Keir Starmer
Cuts will set you free, Fiscal Incompetence Award: Rachel Reeves
Worst co-production Award: Timms PIP Review
Runners Up: Knowledge and Understanding Framework (KUF) training programme.
A provider who churns out “co-produced patient lounges” in inpatient wards like there’s no tomorrow… because patients would all rather choose the colour of a gaming chair than have strategic influence.
Lifetime Achievement Award for Democidal Policies: Iain Duncan Smith
DWP War Criminal of the Year: Joint award to Liz Kendall and Stephen Timms.
Author of ‘The Department’, disabled journalist John has been holding the DWP and others to account for 25 years as the only news agency specialising in disability issues.
Stop Oxevision is a brilliant, thorough, well researched campaign to highlight the use of Oxevision, a patient monitoring system consisting of an infrared sensor and camera, which can be used to observe patients remotely.
One day a woman was admiring my new outfit and smiling, casually said “careful someone might phone the DWP” making a phone call gesture (because of course that someone might be her).
My blood ran cold, in that moment I really disliked that person and will think they’re scum forever. This is not the first or last time this has happened, that people jump to this response in relation to something like nice clothes is disturbing to me but apparently acceptable to others. The fact that I’m on disability benefits is clearly never far from their minds and weaponising it against me isn’t either.
Another time a friend queried whether I should be spending my benefits money (£25) on a massage, y’know shouldn’t it be for things like food and leccy? She didn’t know anything about benefits, my benefits, why I get them or anything else but thats ok she entitled to question me about it.
The idea that they are paying for you so they have the right to police you, that “taxpayers” rhetoric has really worked in a very deep rooted way. Its not my money, its theirs.
Every time this happens I find myself justifying to myself why I bought new clothes, why I bought a massage, why I needed them, because I’m doing it too.
I’ve been investigated for fraud twice, once in the 90s when legislation changed in April and suddenly lots of people where committing fraud so we had to report en masse to the fraud dept. And a second time around 2010, I say second time but it actually lasted for 6 yrs. I was summoned to the fraud dept, was questioned and had to give a statement, I was told “90% of people who come into this room end up in court”. I didn’t, I still have no idea what fraud I was accused of, why and more importantly who reported me. For 6yrs I received constant forms to fill in and random phone calls; someone would say their name really fast, so I couldn’t catch it and then bark questions at me “how much money did I have in my account? How many times I had I been abroad in the past ten years (with outgoing/incoming dates). They always refused to repeat their name or give me any details such as a phone number.
Could you do that? Tell someone how much money you have down to the last penny on demand? Do you have the dates of all your travel over the past decade memorised? Tell a stranger that phoned you without warning?. I had to. This was also information I already provided multiple times.
It was suggested, by welfare rights, that the DWP had a vendetta against me, that it was purely malicious, I had the option to take action but by that point I didn’t want to poke the wasps nest any further. I depend on the DWP for my survival. The harassment abruptly stopped when I moved onto PIP & ESA.
I should add that I’m in the Substantial Risk group as I am “a danger to myself and /or others and must be supervised at all time”. It doesn’t protect you from the abuse of the DWP.
I’ve been dismayed on social media at how many disability benefit recipients including activists suggested in response to the “my Aunty gets PIP but I know shes faking disability” posts, with “Oh you should report her then, that’s on you”. When I suggest “how about we mind our own business” people got very defensive and pissed off at me because I’ve committed the sin of having unwavering solidarity with all my fellow benefit claimants (real or fictional) and perhaps highlighted their lack of.
We are not only conditioned to accept that there is extreme wealth, with all its idleness, greed and corruption, to admire & aspire to it, but also to focus on each other instead, punch down or across, but never up. Focus on the minutiae not the big picture. Across class antagonism is an invaluable, no, essential tool of the state and it will do anything to maintain it.
We are also conditioned to accept that there is extreme poverty, but unlike wealth, it must be monitored, scrutinised and policed. Your neighbour might be spending money on something the state might not approve of. Your poor friend on benefits might be the undeserving kind of poor. Its up to you to decide that, no evidence needed, you must be the eyes and ears of the state.
And so the DWP panopticon has tentacles reaching out into the wider society, we are taught to act in the interest of the state at all times, we become its unquestioning agents. In collusion with and fawning over our benefactors who are also our oppressors. Its so engrained in us that that to question or challenge it is considered itself an act of antagonism, I’ve been accused of policing what people can say because this is also part of the conditioning; to accuse dissenters of the v thing you are being told to do.
We are expected to carry and enact the DWPs pettiness and spite. Poor people against poor people, because are all poor, the taxpayer and the scroungers together, we are all poor and making someone else poorer, won’t make you any less poor.
Its never OK to encourage people to report someone for benefit fraud, not as a joke, not a gotcha, to highlight hypocrisy, to make a point, never. For a myriad of reasons its not ok.
Just mind your own business
It can destroy someone’s life, it can cause someone’s death.
The sense of panopticon, surveillance, fear of getting anything ‘wrong’, being believed, knowing you’re not viewed as disability ‘proper’, viewed as morally deficient, all contribute to increased paranoia, depression, anxiety, self-harm/suicide.
Some people relay how DWP processes, government, and the endless drip feed of derisory media have resulted in this getting embedded into auditory voices heard, persecutory fears, low self-esteem.
“I started to fear the police would break into my home, drag me off and put me in prison”
“I was afraid to stand near my window in case I was under surveillance”
“I can’t go out or speak to people I don’t know, they could be undercover operatives”
“I heard my thoughts in the voice of Ian Duncan Smith”
“I can’t bear receiving post because of DWP letters, I ask friends/relatives to not write to me”
*I have vomited at the sight of an envelope”
“I can’t do a class, socialising, doing voluntary work, in case anyone asks me what do I do. I’m afraid of people knowing I’m a claimant in case they think I’m a scrounger and ring the fraud hotline”
“I have exit plans in case I can’t face the next review or lose it”
“I considered physically disabling myself so that it was visible and I’d be believed”
I just migrated from ESA to UC with LCWRA, I am unable to work due to severe mental health issues, including complex PTSD, complex personality disorder (ie. more than one personality disorder) and an eating disorder. It’s been so much fun reading about what Labour are planning to do to longterm sick and disabled people like me, because it has triggered and/or exacerbated every single one of my existing mental illnesses!
As I often say to my therapist, it is excruciatingly challenging trying to recover from an illness that makes you believe that everyone is out to get you and nobody cares about your wellbeing when the government has proposed cutting your means of survival and the resistance is almost exclusively limited to other longterm sick and disabled people. What makes it worse is that it’s a Labour government this time, ie. the supposed “good guys;” it is starkly different coming to terms with the fact that the people who are meant to be on your side are now targeting you as brutally as the “bad guys” always have, and frankly it has undone much of the progress I had made in dealing with my cPTSD. When you have been through trauma, it is vital to learn to trust people again rather than seeing everyone as “bad,” and yet Labour are supposed to be on our side, so is this not a perfect example of my trauma-injured brain being correct? In which case, how on earth am I supposed to recover when my supposedly skewed mentally ill view of the world is so perfectly aligned to reality?
The allegedly helpful “pathways to work” part of the Green Paper made me laugh; the DWP have literally never been the “good guys,” anyone who’s ever actually had to claim out-of-work benefits and deal with the system knows that already, so it is hysterically naive and out of touch for MPs to believe that the DWP will support sick and disabled people in any way. We live in fear of them, now more than ever.
Moreover, my eating disorder has been much worse since the benefit cuts announcement; as with most EDs mine is about needing to feel like I have control over something when everything else feels out of my hands. Needless to say, hearing that I am one review away from losing half my income has sent me spiralling, and my ED currently is worse than it has been in years. The sheer anxiety of waiting for that dreaded brown envelope to arrive summoning you to explain yourself and your health conditions (often invisible ones) to an unqualified DWP employee has increased tenfold now that the stakes have been raised so high, and you never know when or if it’s going to come, so you can’t live a single day in peace.
I don’t need to tell you how useless the NHS mental healthcare services are, so after they had made my mental health dramatically worse I gave up and went private; that is what I spend my UC on, and of course if the health element is removed from my benefits then there is no way I will be able to afford this healthcare anymore. One could argue that doing this to all the longterm mentally ill people who are currently paying for therapy would put pressure on the NHS once they are unable to afford private support anymore and go back to the NHS, but I disagree; I believe many of us will simply take our own lives at that point.
Only ignorant people would assume we’ll all flock back to the NHS, as if we’re paying out of our meagre benefits money for therapy for fun and not out of sheer desperation because NHS services are worse than useless, more damaging to our mental health than no therapy at all. Without the UC health element, we cannot access healthcare, and consequently one way or another we will probably die. We’ve heard Labour loud and clear with their constant demonising of those too unwell to work, the use of “working people” to explicitly exclude us, and their plans to cut off our means of survival; this government wants us dead, there is no other explanation. Words cannot express what a terrifying and painful experience living with that knowledge is. It would be horrific under a Tory government but to face this under a Labour one is unspeakably cruel.
The Labour Government’s DWP Pathways to Work Green Paper is brutally damaging people’s mental health. Below is one such testimony. If you want to share yours, in confidence, please email
recoveryinthebin@gmail.com
My paranoia has increased dramatically. (Though is it really paranoia if you know they are genuinely trying to remove support from people?) I am afraid to leave the house on days when I am well enough to go out in case a DWP person photographs me or a neighbour reports me for what they wrongly perceive to be ‘fraud’. I am trying to keep my health from worsening and going outside when I’m able, especially to walk, is literally keeping me alive, but since the green paper announcement every day I am frightened to do it.
I live with intrusive images and thoughts which have increased in frequency and severity. My brain compulsively rehearses the scenarios, forcing me to live them out.
One of the most common scenarios now involves being in the DWP office and being interrogated about intimate and embarrassing aspects of my ill health by a complete stranger then being disbelieved when I try to explain, and having all income removed, leaving me destitute. Another common scenario my brain forces me through is me being anxious, distressed or panicked at a benefits review and being mocked for it and dismissed as a liar. (I have good reason to fear the latter, an assessor once laughed at me when I tried to explain how distressed and exhausted I was feeling, and I struggled, and I found it difficult to speak.)
My brain tells me that I am being investigated for fraud, that every time I spend money I am being tracked by the DWP, trying to find reasons to remove my support and force me to try and work. My brain shows me what will happen if I try to work, that the environments and the work itself will make me more and more unwell, that I will spend all my time and energy failing to get to work or trying to get an employer to believe me about how impossible I am finding things, until eventually I collapse or die. I speak out loud more and more to myself, forced to act out these scenarios alone in my home, which is exhausting.
These images and scenarios replay and replay and replay. I have developed some strategies to try and reduce their duration, and to help myself recover afterwards, but since the green paper announcement they are getting harder and harder to manage. I have no support managing any of this because I find it so difficult to make and keep medical appointments, and whenever I’ve tried in the past nothing has really helped, and I am made to feel like a failure. This all adds to the guilt and fear I already feel about not having enough money to live and having to rely on benefits. And it worsens all my other health conditions, mental and physical: fatigue, pain, depression, anxiety.
I wish more people who have never had prolonged contact with the DWP would understand how traumatising the green paper announcement has been for so many of us. I hold no hope that politicians will do the same but perhaps if more ordinary people listen to us they will be forced to hear our voices.
The Labour Government’s DWP Pathways to Work Green Paper is brutally damaging people’s mental health. Below is one such testimony. If you want to share yours, in confidence, please email
recoveryinthebin@gmail.com
Been on disability for 25 years. Was originally in the “Substantial Risk” group. I’m Limited Capability for Work Related Activity (LCWRA) and have been for a long time I also get High rate mobility Personal Independence Payment (PIP) and Standard rate care PIP, moving onto Adult Disability Payment (ADP) this month which will remain the same until I’m re assessed by Social Security Scotland (SSS) in August.
Scotland will lose almost £500 million in social security funding if the proposals go ahead and will have to make similar cuts. But there’s no clarity on that yet. I’ve been diagnosed with several Personality Disorders (PD’s), have been blacklisted by psychiatry, cannot access NHS therapy (but have had plenty in the past). The NHS knows I’ve self harmed since I was a small child. They know I think of suicide, the NHS has no interest in either of those realities. I receive support from a local charity. I have lots of physical health issues; fibromyalgia, chronic fatigue syndrome (CFS), Functional Neurological Disorder (FND), arthritis, migraine etc plenty of the “Dustbin diagnoses”. I receive no support for those either. In some ways the DWP have been more validating than the NHS.
I’m dreading my re assessment in August although it should be easier than the DWP , I’m just so tired. I don’t know if I can face it. I’m thinking about these cuts all the time, it’s always on my mind. Have invested in a large amount of first aid gear as I anticipate an increase in my self harm, which is often life threatening. It hasn’t been a big issue for a while as being finanically secure helps my mental health immensely. If the cuts go ahead I will lose everything, I will be on £49 a week, will be expected to look for work and will be sanctioned if I don’t.
I cannot work. The DWP has said that for 25 years. I will be made destitute, homeless and there will be no way back from it as there will be no safety net.
I will be obliged to die. I’ve already bought the rope, the pills and know what to do. I’ve been researching and practising. I will have no other option. So now I’m a life clock, a suicide deadline, out of neccesity and obligation. Death will be the only option. I’ll wait till I have to, but maybe I should do it sooner and save myself a lot of stress since it’s inevitable anyway. Either way I have no choice. You can see how my head is in a loop. There is no future. I have new serious health issues I need long term treatment for but why bother? They want me dead, seems pointless to give a shit now. Why bother improving my health. I’m not going to the GP or engaging with the NHS anymore, there’s no point, I’m already dead.
The Labour Government’s DWP Pathways to Work Green Paper is brutally damaging people’s mental health. Below is one such testimony. If you want to share yours, in confidence, please email
recoveryinthebin@gmail.com
I get DWP specific nightmares and insomnia waking up at 3am.
Typically my nightmares involve the police and DWP using a battering ram to break into my home at 6am, dragging me off in handcuffs because of a malicious complaint.
Or long range cameras photographing me in my kitchen, or undercover operatives in Sainsbury’s.
My most recent nightmare involved an old GP ringing me up (his voice was spot on), with DWP, insisting I had to start a mandatory work programme, being interrogated on what I do during the day and demanding to know if I could get on a bus, and if I could it would mean I would lose all entitlement.
When I woke up it took me a couple of hours to work out that this hadn’t happened. I had to look at my phone record, check to see if I had messaged anyone. Initially I still wasn’t sure, maybe I just hadn’t rung anyone yet?
It took time to sink in, it was another nightmare.
My nightmares now match my reaction to DWP envelopes – nausea, actual vomiting, lasting panic and anxiety.