This image and words are by Nila Gupta, who is no longer with us. Rest in power Nila.
One of the things I’m feeling a lot at the moment is the massive divide being successfully constructed between:
1. Those of us who are long-term dependent on state disability benefits to live.
2. The rest of society.
This is absolutely deliberate.
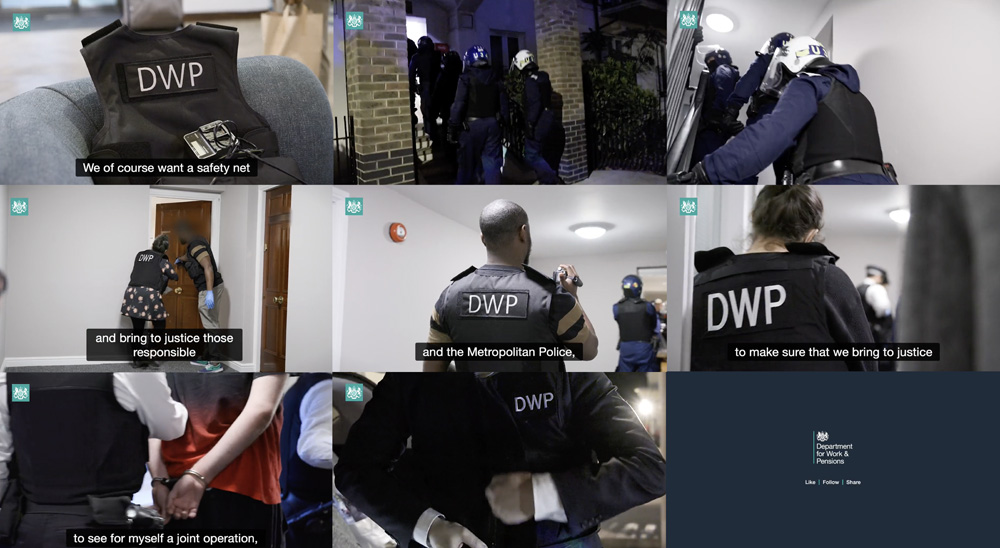
People who aren’t dealing with the DWP for disability benefits have no idea how traumatic and violent and all-encompassing it is. It is an ongoing trauma for a lot of us.
Pretty much everyone I know who, like me, relies on disability benefits for rent/food/bills/life money, has had multiple traumatic experiences. And that’s on top of the GIGANTIC amount of work that the assessment process involves: do to it successfully requires a lot of specialist knowledge, writing skills, capacity for loads of admin, having to contact people, arrange medical appoints which are a total waste of patient and NHS resources, attend horrific ‘assessments’ , try to find advocacy etc
And being forced to do this all to the tightest timescale possible.
We deal with a level of surveillance and arbitrary punishment that, rightly,
has been judged by multiple independent analyses to be a state driven deliberate breach of the human rights of disabled people who have the fucking gall to be poor and/or unable to work.
Loads of the techniques of psychological pressure were developed first in one of the home office/ foreign office/ DWP, and then exported to the others. Nice, huh?
If you’ve a strong stomach and/or are not directly affected, more on that here.
“Nudging conformity and benefit sanctions: a state experiment in behaviour modification“
Basically the gist of this is, in which we discover until recently there really was a controversial government department which researched and tested “behaviour modification techniques” for implementation in aggressive state policy:
“Conservative anti-welfare discourse excludes the structural context of unemployment and poverty from public conversation by transforming these social problems into individual pathologies of “welfare dependency” and “worklessness.”
The consequence is an escalating illogic of authoritarian policy measures which have at their core the intensification of punitive conditionality. These state interventions are justified by the construction and mediation of stigma, which is directed at already marginalised social groups that the policies target. The groups, which include sick and disabled people, people who are unemployed, are painted with a Malthusian brush, as a “burden on the state” and a drain on what are politically portrayed and publicly seen as scarce resources in an era of austerity.”
Political processes of scapegoating, stigmatisation and outgrouping have been amplified by a largely complicit UK corporate media. Examples of its work are all over the DWP. PREVENT. The whole Hostile Environment project. There’s plenty more, I’m sure.
Which is why I’m not exaggerating when I name this as state terrorism.
A bunch of disability and civil liberties activists/campaigners/lawyers discovered the existence of the ‘nudge unit’. So they made Freedom of Information requests to try and find out what the hell government money is being spent on.
Government solution? To privatise the department and turn it into an ‘institute’ to avoid scrutiny. And to drain more state cash into private pockets.
Anyway, back to us, trying to survive in an increasingly violent and reactionary society with the vast machinery of the right wing state bearing down on us.
This shit and much more stuff like it = many of us are scared to leave the house, post any pictures of us looking happy on social media, be photographed at events/protests.
We’re cut off from participating in civil society.
Police force admits agreement to share information about protesters with DWP
It’s absolutely deliberate: the more surveillance, the more the DWP poke their nose and disclosure agreements into every area of our lives, the scarier it is to be out in the world even when we aren’t disabled by society.
And – for many of us – there are multiple other oppressions we’re dealing with too. Disability is inextricably entwined with race, class, gender, gender id, immigration status, sexuality and poverty.
Our lives are FUCKING HARD.
The surveillance/sanctions regime is a deliberate tactic to put extra pressure on already vulnerable people. It’s punishment for being vulnerable and in need. It’s also eugenics: it’s about disabled people being regarded as disposable/barely/not human. It’s an idea with deep roots in British society.
And they’re only just getting started. Looking at Bloody Boris’ fucking cabinet terrifies me, eg right now the DWP is trying to get its hooks into NHS files. The proposal is dressed up in fake nicey language but basically it would mean that if you claim disability benefits, you have no privacy or confidentiality during medical appointments. It would be horrific. I know that there’s a lot of pushback against this from loads of NHS groups, thank fuck.
I don’t have much hope, and I feel a lot of the time the clock is ticking on how long I can survive before they break me, or make me homeless again or otherwise fatally fuck me up. That worry never leaves me. Which is another reason for stopping dealing with them for now.
Because I realise now: I’ve become institutionalised. I live inside an invisible cage built by the DWP (and Social Scare, of course. Let’s not forget them. Bastards)
By institutionalised, I mean, for eg – I anticipate and strategise against DWP sanctions automatically whenever I think, open my mouth, and especially if I leave the house. Any time I think about doing anything out of the house that might improve my life, (eg an art class, or an event that a photographer is at) I freak out over whether it will trigger sanctions.
Because although it’s not likely, it does happen.
It’s a perfect panopticon. They fuck over just enough people to make all of us realistically terrified about it.
And it’s a deliberately and increasingly asymetric system.
Ie: getting the benefits takes huge amounts of work, and can take years. But the state can take them away in an instant.
There’s also the alienation: I deal with this monster that infests every area of my life. People who don’t deal with it mostly have absolutely no idea how hard our lives are. How we don’t go a week on social media without hearing about yet another death caused by the system we’re reliant on.
A system that is our right.
And it should be the right of anyone living here, btw. And isn’t anymore – that’s a whole other pile of DWP fuckery that’s been happening over the past decade or so.
Fuck borders and fuck nativist politics always.
But my one hope is that I see so many grassroots people/groups/organisations/communities doing mutual aid, advocacy, support, skill sharing etc. A lot of it is very informal and grassroots and it’s amazing. So you get people on random fb forums putting hours into helpful /detailed/informed responses to questions. You get people sharing often traumatic details of the assessment process because they care about someone else going through the same thing. It’s fucking amazing. But we shouldn’t fucking be going through this shit in the first place.
More specific stuff re the ”invisible cage’/panopticon:
CW: moar DWP ranting. Also, tho, theory.
Which isn’t actually fucking theory for me. It’s my daily life.
The DWP is absolutely a panopticon. I’m living in a fucking panopticon. Except it’s invisible. And specifically designed to marginalise already vulnerable people.
So most people don’t even know it exists. And often don’t believe you when you tell them. And it fucks you up so sometimes* you forget that you’re living in a panopticon and just blame/hate yourself.
I’m living in a panopticon in twenty fucking nineteen in a rich White Western country that likes to think of itself as:
1. Liberal (it isn’t. There are important traditions of liberalism in this country. Traditions of radical internationalist anti colonial/anti racist socialism, communism, anarchism. Powerful histories of working class people of all races doing practical radical political work. And loads more. Britain’s dominant character as a ‘nation’ in general, in practice ends up defaulting to English norms’ . Which prize conformism, hierarchy, subtle powerful coded signals.
Its all about us ‘knowing our place’.
Riz MC nails it in ‘Englistan’:
“God save the queen
Nah she ain’t mates with me
But she keeps my paper green
Plus we are neighbours see
On this little island
Where we’re all surviving
Politeness mixed with violence
This is England”
Track: Riz MC Englistan on Bandcamp
Lyrics: https://genius.com/Riz-mc-englistan-lyrics
2. Modern. Modernity isn’t inherently good – in English, it’s a category inseparable from white supremacy and capitalism and patriarchy and and and.
But my main issue is that the idea that the UK is modern is fucking laughable. UK = basically feudal neoliberal empire-hangover capitalism. Doesn’t that sound just GREAT?
If you think I’m exaggerating – bear in mind that our new Prime Minister is related to the royal family. In twenty fucking nineteen.
Thinking about the DWP as a panopticon also usefully reminds me that there’s a reason that a fucking White English public school-and-oxbridge man came up with with the panopticon. These same people still largely run the country OVER TWO HUNDRED YEARS LATER.
“Jeremy Bentham, an English philosopher and social theorist in the mid-1700s, invented a social control mechanism that would become a comprehensive symbol for modern authority and discipline in the western world: a prison system called the Panopticon.
The basic principle for the design, which Bentham first completed in 1785, was to monitor the maximum number of prisoners with the fewest possible guards and other security costs. The layout (which is depicted below) consists of a central tower for the guards, surrounded by a ring-shaped building of prison cells.
The building with the prisoners is only one cell thick, and every cell has one open side facing the central tower. This open side has bars over it, but is otherwise entirely exposed to the tower. The guards can thus see the entirety of any cell at any time, and the prisoners are always vulnerable and visible. Conversely, the tower is far enough from the cells and has sufficiently small windows that the prisoners cannot see the guards inside of it.
The sociological effect is that the prisoners are aware of the presence of authority at all times, even though they never know exactly when they are being observed. The authority changes from being a limited physical entity to being an internalized omniscience- the prisoners discipline themselves simply because someone might be watching, eliminating the need for more physical power to accomplish the same task. Just a few guards are able to maintain a very large number of prisoners this way. Arguably, there wouldn’t even need to be any guards in the tower at all.”
“Michel Foucault, a French intellectual and critic, expanded the idea of the panopticon into a symbol of social control that extends into everyday life for all citizens, not just those in the prison system (Foucault 1970). He argues that social citizens always internalize authority, which is one source of power for prevailing norms and institutions. A driver, for example, might stop at a red light even when there are no other cars or police present. Even though there are not necessarily any repercussions, the police are an internalized authority- people tend to obey laws because those rules become self-imposed.”
* ie almost all the time.
A final thought:
The tories are trying to kill me.
And a LOT of other people.
And they’ve already killed so many.
Black people. Muslims. People of Colour.
Migrants, particularly guess what, black people, muslims, people of colour.
Disabled People. Mad people.
Trans* people
Queers
The ‘wrong kind’ of women.
Working class people
*
Think about what it’s like for those of us who tick most or all of these boxes.
Try to conceive of the firestorm that we’re living in.
quotes are from here Internalized Authority and the Prison of the Mind: Bentham and Foucault’s Panopticon
Recovery In The Bin (RITB) is covered by a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International(CC BY-NC-ND 4.0)
License