Open Letter to some of those attending the Global Disability Summit
To:
Lenin Moreno, President of Ecuador
Gabriela Michetti, Vice President of Argentina
Sophie Morgan
20 July 2018
We are writing this open letter to you on behalf of Deaf and Disabled people across the UK concerning your involvement in the global disability summit being co-hosted by the UK government in London on 23 and 24 July.
We are strongly in favour of international support that improves the lives of Deaf and Disabled people across the world and welcome co-operation between States that lead to stronger human rights laws and protections. We particularly support the building of international solidarity and links directly between Deaf and Disabled People, our organisations and campaigns.
However, we have the following concerns regarding the July summit:
The role of the UK government in co-hosting the event. Following an unprecedented investigation carried out by the UN disability committee under the United Nations Convention on the Rights of Persons with Disabilities (UN CRPD), the UK was found responsible for grave and systematic violations of Disabled people’s rights due to welfare reform. The findings of their investigation, published in November 2016, were and continue to be entirely dismissed by the UK government. In August 2017 the UK government was routinely examined under the UN CRPD and again the UN disability committee expressed their deep concerns regarding the UK government’s failure to understand the Convention, the impact of their policies and failure to recognise them. Again the UK government said they disagreed with the findings of the Committee. The involvement of the UK government in co-hosting the summit therefore undermines any aims of the summit linked to strengthening Deaf and Disabled people’s rights under the UN CRPD. Instead it provides a platform for them to showcase to other States how it is possible to get away with ignoring those rights when it comes to your own citizens.
The UK government’s use of its international work to cynically deflect from criticisms of their disability record in the UK. On a number of occasions when government ministers have been criticised for implementing policies with an adverse impact on Deaf and Disabled people, they have cited the poorer conditions of Disabled people in other countries. This represents a misunderstanding of the UN CRPD which is about the progressive realisation of rights. The UN disability committee have such concern about the situation in the UK because it represents a serious and dramatic retrogression of rights, described by the Chair as a ‘human catastrophe’. In deflecting attention from their record in the UK, the Government clearly intend to more easily continue their punitive policies targeted at Disabled people and the poorest members of society. There is now overwhelming evidence, evidence which the UN disability committee considered, that prove the brutal impacts of these policies. It would be a betrayal to all those suffering under them not to raise concerns about attempts such as use of the global summit to divert attention and opposition to those policies.
The suitability of the Government of Kenya as co-hosts given their abuse of the rights of LGBTQI+ people, many of whom develop lifelong impairments as a result. LGBTQI+ people in Kenya are routinely banished from their families, denied work and accommodation, imprisoned and persecuted. They face severe barriers to forming and maintaining relationships and to living as a couple, the ‘Right to Family Life’ that every human is promised. This results in widespread damage to their mental and physical health, creating impairments where none previously existed. This is reflected in the high level of asylum applications to the UK from LGBTQI+ asylum seekers from African countries.
Despite their experiences, the majority are then refused asylum in the UK and forcibly returned home, where many disappear or are murdered. Just this April, President Kenyatta said that LGBT rights are “not acceptable” and not “an issue of human rights”. The Kenyan Government has also claimed this is a non-issue for Kenyans, and no doubt would argue that it has nothing to do with the Summit. However, if you are Kenyan or Ugandan and are lesbian, gay, bisexual, trans, queer or intersex, it is an issue that completely dominates and dictates your life. For many Disabled people from Kenya, it is the reason they developed an impairment in the first place. Under the UN CRPD, the Kenyan government also has an obligation to protect the rights of disabled people who are LGBTQI+. We appreciate that you may not have had this information when you agreed to involvement in the summit and would be happy to meet to discuss our concerns. Please do not hesitate to contact us with any questions or for further information.
RITB (Recovery In The Bin) members have intersecting identities and social positions such as BME/LGBTQIA+/people in receipt of social security. We are a group of people marginalised in many ways, not just because we are mental and disabled by society. We especially wish to stand in allied solidarity with these groups and condemn racism, transphobia, homophobia, sexism & scrounger rhetoric. We call on liberation movements to stand in solidarity with us.
If you wish to add your name or org to this statement please email the details to
Crisis Houses: An alternative to Hospital Admission? A look at real world crisis houses at Tees, Esk and Wear Valley NHS Mental Health Foundation Trust.
Up North the Durham & Darlington Crisis house run by Tees, Esk and Wear Valley MH Foundation Trust has been sitting empty since December 2017 while service users aren’t informed it exists. Is this TEWV’s way of maintaining the hospital/medical model status quo by ensuring Crisis Houses are destined to fail, or is it something to do with Crisis House model itself?
The current UK government’s review of the Mental Health Act is placing strong emphasis on reducing detentions. As such, better community services including support in a crisis are high on the agenda with strong calls to introduce more services that support people in acute distress outside the hospital environment. (1)
The question is whether such services would be effective and safe for patients and provide genuine alternatives to hospital. When crisis teams were introduced they too were intended to be a service for people who would otherwise be admitted to hospital. The course of time has shown that suicide is far higher under crisis teams than in inpatient care (2). Nevertheless, steps are being taken to improve community based services.
‘Crisis Houses’ are one of the options frequently mentioned in debates around better community services in crisis and alternatives to hospital. But do we know what would happen if crisis houses were rolled out on a wider scale?
Recently Recovery in the Bin were told about a consultation by Tees, Esk and Wear Valley NHS Mental Health Foundation Trust on the continuation of their County Durham and Darlington Crisis House which opened 4 years ago. The consultation highlighted that an inpatient bed costs the Trust £380 per day whereas a Crisis house bed cost the Trust £480 per day, though the consultation doesnt mention effectiveness – and cost -effectiveness – of shorter stays in the Crisis House than hospital. The sobering figures showed that very few service users were considered ‘appropriate’ for the Crisis House. Admissions were via the crisis team and the Crisis House had in fact been closed since December 2017 with not a single referral accepted and the staff working elsewhere in crisis services. Unsurprisingly the Trust wanted to ‘review the role and function’ of the Crisis House.
We felt more information was needed on the circumstances behind this situation and asked a member of our group who is under the care of the Trust to find out more.The Trust provided further information as follows:
Question 3. How have you determined that the lack of referrals to the crisis house are not a result of overzealous gatekeeping? Trust Response: The crisis and recovery house provides an alternative, safe, supportive environment for intensive home based treatment for those experiencing a period of acute distress and who would benefit from a planned period of time away from home. The service is not used as an alternative to inpatient admissions and is not an element of the gate keeping process.
Question 6. How many service users have the crisis house on their care plan or have been informed it exists? Trust Response: Service users are made aware of the crisis and recovery house service, if and when it is appropriate to their care and treatment. As admission is made directly from the crisis teams based on immediate need, it is not identified within individual’s crisis plans (part of the overall care plan).
Question 2. How have A&E attendances for mental health problems changed during the 4 years the crisis house has been open? Trust Response: The crisis and recovery house does not provide emergency mental health care services. As such, we would be unable to ascertain any correlation between the service and A&E presentations.
Not all questions were answered (a FOI request may be needed) and we felt the responses that were received raised more questions.
While it is probably obvious to readers how insufficient the Trust responses are we nevertheless spell it out below.
The Trust replied that the Crisis House is not an alternative to hospital admission. Their consultation documents, in contrast, say the crisis house provides ‘an alternative..for intensive home based treatment’ and then explains that intensive home based treatment is ‘an alternative to hospital admission’. It seems somewhat illogical to consider the house not to be an alternative to hospital admission.
The Trust’s reply dismisses the possibility that the empty beds at the Crisis house may be a result of overzealous gate keeping. Yet it also claims all admissions are via an assessment by the crisis team when a service user is in acute distress. In fact, service users are only informed the crisis house exists if the crisis team decide that the house is an appropriate option. It is difficult to imagine a clearer example of impossible to challenge gatekeeping.
The Trust makes clear the Crisis House is not included in advanced crisis planning for known service users – it is not put on crisis plans for example. This seems somewhat contrary to the principles of the crisis care concordat. Furthermore, it calls into question the Trust’s consultation documents which claim that admissions to the crisis house are ‘planned’. A service user in acute distress informed of the Crisis house as an option following assessment by the crisis team is unlikely to experience much delay between assessment and admission to ‘plan’ admission to the house.
The Trust, which is consulting on the function and role of the Crisis House, claims they cannot ascertain any correlation between the Crisis house and A&E attendances for mental health problems on the basis that the crisis house does not provide emergency mental health services. But the Crisis house is designed to provide intensive home based intervention – which is an alternative to hospital admission for people in mental health crisis. The purpose of crisis planning is to prevent mental health emergencies. In addition, the consultation specifically pinpoints psychiatric liaison services as one of the reasons why there has been a reduction in the use of the Crisis house and yet psychiatric liaison is a service that receives referrals from A&E and may divert service users toward the crisis team. A&E attendances for acute mental distress and service users in crisis are essential for understanding and evaluating the role, function and impact of a crisis house.
This ‘case study’ of community based crisis services raises a lot of questions for TEWV to reflect on about the standard of crisis care and crisis planning they deliver and the extent to which they involve service users in decisions about their own care. It also raises questions about the effectiveness of consultations with patients and the public by NHS organisations, especially the quality of relevant information given to ensure stakeholders are enabled to provide fully informed opinions.
Over and beyond these considerations however, there is the wider question of how community based services might be implemented in practice if the drive to reduce detentions continues to call for greater emphasis on support outwith the hospital. And will service users ultimately benefit?
Is TEWV crisis house typical or are crisis houses working better elsewhere? What ensures the model works and why, at TEWV, has it resulted in a farcical scenario, reminiscent of 1980s satire Yes Minister (3), where patients around the country cannot get hospital beds but at TEWV an entire crisis house is sitting entirely empty?
According to the Royal College of Psychiatrists, “Liaison Psychiatry is the sub-speciality which provides psychiatric treatment to patients attending general hospitals, whether they attend outpatient clinics, accident and emergency departments or are admitted to inpatient wards. Therefore, it deals with the interface between physical and psychological health.” There is a ‘Faculty’ for Liaison Psychiatry at the RCPsych and they are running a pilot to develop a credential in Liaison Psychiatry.
The academic and training view of RCPsych is a world apart from my experiences of Psychiatric Liaison in my local Accident and Emergency, (A&E) department. I am emerging from a mental health crisis which involved at least 12 visits to A&E and minor injury units within the space of just several months. I self-harm by cutting my body as a last resort during times of extreme distress. The self-harm is not ‘addictive’ in nature but it is incredibly painful. I harm for the need to get this act over with in order to have a chance to feel better later. I feel compelled to cut and displace the distress, thereby enacting deep inner pain which is beyond words. In the past I have needed surgeries, multiple blood transfusions and countless stitches. Attendances at A&E have been only the tip of the iceberg of my self-harm and it has been far more usual that I go to see the nurses for wound sterristripping at my GP practice or self-treat.
If Psychiatric Liaison does bridge the interface between physical and psychological health then I may seem an ideal candidate for its expertise. My self-harm does have physical complications, not least iron deficiency anaemia and open wounds that take time to heal. I welcome advice, practise harm minimisation and am crying out in pain during a cycle of self-harm. Recently when cutting one area of my body I hit major veins and the blood loss necessitated ambulance call outs. After the second ambulance I decided to avoid harming this area of my body as I don’t want to bleed to death. I am resolved to reduce the harm and minimise my ‘impact’ on local overstretched health services.
I must report that my experiences with Liaison Psychiatry have added insult to injury. A ‘good’ visit to A&E involves not only physical treatment with adequate anaesthesia, but the treating medical doctor agreeing that I don’t need to be referred to the Liaison or Crisis Team, (the Team which is on call depends on the time of day or night). I explain that I have seen the Crisis Team and Psychiatric Liaison in the past and they have nothing to offer. I usually wait hours in the department for the Liaison Team to come on duty or finish with other patients then they permit me a ten minute chat. This chat usually consists of asking why I am there, was the self-harm superficial, (would I be there if that was the case I wonder?), have I tried counselling and how will I get home?
The Liaison practitioner may feel the need to draw up an action plan which will say something like ‘aware of crisis numbers.’ Since the crisis numbers such as the Samaritans and the local mental health helpline are widely available I don’t need to be given them. I don’t see why I should have waited hours on top of the prior three hours wait for physical treatment for this unnecessary assessment which will just tick a box for the service.
My resistance to Psychiatric Liaison probably relates to the fact that they work for a mental health trust which discharged me in 2015 by saying they would not see me again while I had the ‘same presentation.’ Since I have no history of psychosis I am not sure how I can morph into a different presentation which would be more agreeable to the mental health team. Over 16 years ago I was given a diagnosis of Borderline Personality Disorder and this still follows me around even though no-one ever reviews it. Previous GPs have made referrals to the ‘Access Team’ which get batted back with conversations with the GP along the lines that I should ‘take responsibility’. I have worked full-time for the last seven years and pay to see a private psychologist.
I don’t know what else I can do to prove I am ‘taking responsibility’ except perhaps drop off the radar of all health services. Sometimes my death would seem like a better outcome to mental health services than my attempting to ask for help that doesn’t exist. I know that Psychiatric Liaison presents a dead end since they have no services to refer into which wouldn’t be hostile to that referral. My local mental health trust is taking part in the ‘Open Dialogue’ pilot but this approach, which comes with much praise for its innovation, would never be open to someone in my type of crisis.
My recent experiences of Psychiatric Liaison have confirmed my misgivings about this service area. I was referred to Psychiatric Liaison by a very thorough medical doctor in June. The doctor spent over an hour suturing wounds. He even said that he didn’t like to see those kind of wounds on anyone and believed that I deserved help and that services had changed, with new options available, since they had discharged me several years ago. He asked if I was under a psychiatrist and I said that I hadn’t seen one since 2013 and services would have no desire to help again.
But in the spirit of being a co-operative patient, and truly being grateful that he did bother, I went along with the referral. The problem was that it was 11.30 pm on a Saturday once the physical treatment was over. The doctor escorted me to the Clinical Decision Unit in the hospital to wait for the mental health team. I then endured a nine and a half hour wait sitting in a chair for psychiatric ‘assessment’.
I would expect the Crisis Team to cover at night where Liaison are commissioned to operate from 8 am – 8 pm. However, it seemed like the Crisis Team didn’t want to come to the hospital that evening and I had to wait for Psychiatric Liaison to arrive on shift on the Sunday. I was seen at 9.15 am by an Occupational Therapist and another quieter unknown team member who chatted to me for ten minutes. I explained I was very distressed and needed to get home. I am a key contact for an elderly parent who would wonder where I was since I hadn’t phoned her that day. The OT still insisted on ticking boxes by talking and drawing up an action plan. I signed the action plan rather than waiting for another ten minutes she said it would take for her to write out this plan.
I was never sent a copy of the plan and have no idea what I signed. I imagine that the plan may have said that I had the crisis numbers and was to go back to work. There was no apology for the nine and a half hour wait in the chair or understanding of the distress and total lack of sleep this had caused. I had tried to self-discharge during the night but had been told by medical staff that the A&E doctor had been worried enough about me to call the police if I left the hospital. Since I have no wish to waste police resources I figured I would need to stay no matter how uncomfortable.
On my next two A&E visits I did see a consultant psychiatrist which seemed unusual given the community mental health team operates with locum psychiatrists and has had no consultant for many years. I was initially impressed by the consultant who had read notes I made in 2015 saying I didn’t want to see Liaison due to the long waiting time which led nowhere. My second meeting with him was less thoughtful due to his assumptions. A friend had accompanied me to A&E and the psychiatrist seemed more interested in talking to her about what she felt was behind my behaviour rather than asking for my account. The psychiatrist said that they didn’t want to make it ‘too comfortable’ for me to attend A&E or they were ‘enabling’ me. I tried to explain how I didn’t enjoy attending A&E and was going for clinical reasons, ie a wound that needed closure through stitches and not because I was a bit upset.
My friend did voice that she thought I needed help from services. The psychiatrist, who was meeting me for only the second time, said that the community mental health team couldn’t help someone like me as they only saw people with a chemical imbalance and were better when there was a clear goal like a medication review or getting someone into voluntary work. The psychiatrist said he didn’t think I was someone who needed to be on medication. He also decided that he would have a professionals meeting to come up with a ‘plan.’ He intended to contact my GP and a primary care nurse who I met only twice two years ago. My private psychologist knows me extremely well but he didn’t contact her at any stage though I supplied her mobile number and email address.
The psychiatrist then said that I wouldn’t see him again even if I went to A&E and he wasn’t my therapist. I asked the psychiatrist for sleeping tablets but despite being based in an A&E department he wasn’t able to prescribe any! He instead faxed a plan to my GP suggesting he ‘considered’ a 14 day course of zopiclone at the lowest possible dose. I tried to explain that I have no history of dependency on medication yet still it felt as though I was asking for hard drugs. Thankfully my GP prescribed sleeping tablets and a tranquiliser without questioning my motivation. I use this crisis medication very sparingly.
The psychiatrist also told me that I should go back to work, this was despite my being physically depleted at a level where other patients may be transfused and at risk of my problems spilling out to colleagues in my distress. I only took one week off work but again it was as though no-one except my GP and psychologist recognised the need for me to do this and spend time with supportive friends. The psychiatrist discharged me to a crisis café which is operated by a voluntary sector organisation and only open for two evenings a week. The crisis café does not offer emergency appointments but feels to me like an extension of their day services which have been reduced by funding cuts.
Since these encounters in A&E I have gone instead to a distant Minor Injury Unit for treatment where I won’t have to see Psychiatric Liaison. These units are nurse led and can perform stitches. However, since stitches take a long time the two nurses on duty will use stapling instead. The staff advise that local anaesthetic isn’t needed with staples but I have felt immense pain when wounds were washed then stapled without any pain relief or anaesthesia beforehand. I feel that Liaison is being used as a deterrent to keep people like me out of A&E yet the consequence is that we will instead have to find other urgent care settings willing to treat us.
When I visited the crisis café one of the paid workers said that a member of the Psychiatric Liaison team had visited the café to say that they are focusing on trying to reduce the number of A&E attendances for mental health reasons as there are too many when A&E is under pressure. My view is that a crisis café which is open for eight hours a week isn’t going to offer a real alternative to A&E and statutory services for someone in acute crisis involving active self-harm or suicidal feelings.
One of the alternatives I used during this crisis was a London A&E department. This experience was a more extreme example of Liaison being used as a deterrent. On being referred after stitches by the doctor to Liaison I was taken to a separate area of the hospital where there were bare rooms with security guards outside them. I was searched and patted down, including my breasts being touched without my consent, by a member of staff who confiscated my bag containing all belongings such as my keys and mobile phone. I was then given a blanket and told to lie down while waiting for someone to see me. I hadn’t eaten, drank or been to the toilet in six hours and I felt terrified. It felt as though I was being detained like a suspect in police custody.
The Liaison nurse did see me after 30 minutes and was extremely apologetic during our ten minute chat. She said that all A&E departments in London were like this as it was their ‘protocol.’ She recognised that I wouldn’t go to this hospital ever again. I needed to use friends and my psychologist to deal with a traumatic stress reaction I experienced within the next few days. I blamed myself for ending up in this A&E and having this reaction, even though it was a London walk-in centre that had sent me there as they couldn’t perform the stitches I needed.
Psychiatric Liaison as a service development needs to be clear about its practices including not using de facto detention in hospitals, such as threatening to call the police or positioning security guards outside bare rooms. This type of detention is illegal without formal sectioning. The assessment should be voluntary and advocacy services are really needed. I see no benefit of Liaison services to people who recurrently self-harm and cannot access help in the community other than by paying for this. However, I can see that Liaison may be able to signpost those with drug or alcohol addictions to treatment or to assess an elderly confused patient for dementia.
I did have one helpful experience in 2015, and I wrote to the Trust to give a compliment, where I was on a ward for surgical debridement and closure and the psychiatrist had visited me on the ward then liaised with the surgical team about my needs. The psychiatrist had been encouraging about the progress made over the years and of the view that secondary care services should offer support. While commissioners are investing money in Liaison there should be clear outcome measures and user involvement in the approaches offered. There should be brief interventions not just a one off chat amounting to ‘how will you get home?’.
The Deliberate Self-harm Team, which was eliminated at the local hospital when Psychiatric Liaison came into being, did offer problem solving meetings and handed out a first aid kit for self-harm which ensured clean blades were used and thick sterristrips were tried at home. This dissolved team did at least have a clear purpose and understanding of those attending who do external self-harm.
I would suggest that Frequent Service User Managers for A&E also offer a more meaningful service. Fortunately, I do have a care-coordinator through a high intensity service user project funded by the CCG. The role of this specialist nurse is to meet people whose attendances have hit a certain threshold and to understand the root causes of their presentations to A&E. She takes a holistic view and understands that crises can be triggered by many social factors such as benefit sanctions, financial, housing and work problems. This nurse has given me a mobile number and suggests I call before things escalate. She has accompanied me to meetings with the HR manager at work given the recent crisis was triggered by my job.
She has also visited the police station when a neighbour’s antisocial behaviour put me on edge. She is not at all punitive, shaming or deterring me going to A&E and recognises that until recently I hadn’t attended for over 16 months. Instead she recognises that the A&E visit is necessary and I know myself best, but to suggest other options which may also help before reaching that desperate point. With her input, I have developed a care plan for my self-harm for the GP practice which indicates my choice of dressings and the nurses’ need to understand that I am in pain with injuries.
I am very grateful that this specialist nurse was also able to ask Psychiatric Liaison not to arrange a professionals meeting and for a note to go on my A&E records asking that I am not to be referred to the Liaison team unless I request it. I don’t think this note on my records is ideal given I am in huge distress when I do go to A&E, but it is a means of saving me further distress in being exposed to psychiatric assessment for no purpose. Harm minimisation can apply to steering clear of pointless ‘interventions’ as much as it can to avoiding life and limb threatening injuries.
There is a risk of referral to Psychiatric Liaison raising hopes of help available to those who self-harm or are suicidal. I guess I have reached the point of knowing this help doesn’t happen so hope is futile. This is another reason why referral should be considered and not automatic as it is a false expectation of help. A ‘plan’ won’t pay for my psychology sessions as I find myself having to apply again for Personal Independence Payment.
A ‘plan’ doesn’t provide a support service instead it is another message that this is ‘all down to you’. I have found the medical staff far more compassionate and helpful than Psychiatric Liaison so I don’t see that the Liaison staff have a training role to do in the department.
I am always apologetic to medical staff in A&E and ashamed of my presence there yet the medical staff are usually saying that I should attend if I have a wound that needs proper closure. The timing of the psychiatric assessment, after long waits for physical treatment, is also misplaced given tiredness and pain may make going home the best option.
I hope that there can be debate rather than gratitude for Psychiatric Liaison as its rolled out to all general hospitals. Psychiatric Liaison in its current form could just be adding to the pain.
Rita Binns
This is covered by a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) License
The idea of disability, when applied to blindness or an inability to walk, seems fairly straightforward – a simple recognition of difference. But its application to mental distress and psychological conditions seems much more vexed and controversial. This is so amongst both health professionals and the people to whom it might be applied. Why might that be?
Disability has a legal definition. In England, Wales and Scotland the Equality Act 2010 covers work, education, housing and the provision of goods or services. At least in theory, the Act protects people from being discriminated against because of certain protected characteristics such as gender, age or disability. To count as disabled you must show that your condition has a “substantial, adverse, and long-term effect on your normal day-to-day activities”. Many of us will feel we easily meet this condition.
There are several ways of looking at disability.
In the medical model, something is wrong with your “body” (and by extension, your “mind”). You have a mental “illness” or “impairment” which disables you from reaching your full potential.
In the social model, something is wrong with your society, and the arrangements it has made for you. Society is what disables you from reaching your full potential. This model does not necessarily value one kind of life over another, treats people as inherently diverse and allows for a variety of attitudes to our condition. (Although many of us are indeed in distress and desperate for a way out, others accept the way we are and do not necessarily want to be “cured” of anything!).
In the case of mental distress and “ill health” both these models are under attack from a third, neo-liberal recovery model.
For some years now, Government policy in the UK has been dominated by “Austerity”: a programme of reductions to public spending and removal of any constraints on business which interfere with making a profit. Profit is assumed to be the highest good and nobody has any “right” to payments from public funds, not even if they contributed the money via taxes and national insurance in the first place. Austerity lies behind the “Hostile Climate” experienced by the poor in general and by some groups in particular (refugees/asylum seekers, members of ethnic minorities and disabled people – above all, those whose continued existence might involve a cost on the public purse).
Neatly fitting into this context, the Recovery model firmly rejects any concept of permanent or long-term psychological impairment or difference and concentrates on finding quick, cheap fixes which get people back to work. It’s important to clarify what kind of work. Ideally full-time and paid, it certainly doesn’t mean work which provides you with enough to live on, or which is socially useful or “meaningful” in some way. The defining feature is that it must make a profit for somebody else – preferably a large employer.
In this model lack of effort (and too much help from family or society) is what disables you from reaching your full potential. Psychological disability becomes essentially a moral question, much as it was back in the days of demon-possession and sin. Although by no means all NHS mental health professionals agree with this view, most in the UK have had to deal with it one way or another. Many feel obliged to pressure people to “recover” in these terms, as rapidly as possible.
So given that the Equality Act gives disabled people rights and a protected status, why might we be reluctant to call ourselves “disabled”?
We may feel we have no right to claim the label, and feel embarrassed at the need for support it seems to imply. (It took a GP’s recognition that her condition was long-term before the writer felt she had permission to use it, for example.) This is of course nonsense in a social animal like homo sapiens whose daily survival depends on the support of others, but in a society dominated by neo-liberal ideas, “independence” can sometimes feel like a necessary condition for self-respect and dignity.
We may associate it with hopelessness, rejection, degradation and despair. Lurking just behind the shoulder of many of us (especially those aged 50+) is the nightmarish spectre of the old “hospitals” where the mentally “ill” (such as unmarried mothers, or those who had accused powerful people of abuse) the learning disabled and the physically disabled alike were incarcerated, lobotomised, electroshocked, raped, abused and/or abandoned and forgotten for ever. (Because of this, for some of us it took a significant act of courage to “come out” to the NHS as “mentally ill” in the first place.)
In the Hostile Climate, where disabled people face routine hostility, harassment and physical attack, it may be genuinely dangerous. Bullying and abuse from others often makes our psychological distress worse. It may even place us in immediate physical danger.
So why might we want to use the term “disabled”?
Many of us fit the definition in the Equality Act, and we may want to claim the legal rights it gives us. Especially if we are in paid employment, we (or our union representatives) may be able to insist that our employers make reasonable adjustments to enable us to continue working on equal terms to our workmates. (I am assured by Unison colleagues that this still can and does happen on occasion, especially in what remains of the public sector.)
It may help others take our condition seriously, and to accept that we’re in there for the duration. It may help to prevent idiocies like telling the severely depressed to cheer up, or trauma victims that there is “nothing to worry about”.
It may help us to insist on our human dignity. It may help us to make common cause with others who face different problems, but the same oppressor. It may help us to build solidarity. It may help us to take ourselves seriously. I like this quote from one of our members, ‘I am disabled due to my emotional distress, adversity, finances and society. Proud to call myself disabled!’
It’s co-production week! Here is a handy how-to for any service users, survivors or otherwise-identifying loonies thinking about getting involved with their local NHS trust or research organisation.
1) Be mad enough that your lived experience of madness can be co-opted and used for foreign-to-you agendas.
2) At the same time be responsible and composed enough to hold down a service user representative’s job.
3) Be very, very reasonable. Do not show any emotions when discussing services you rely on to keep you alive and/or services which have traumatised you so much you want to die.
4) Likewise, do not display any emotion when you are exposed to a constant stream of micro-aggressions and attempts to silence. This is called “being professional”.
5) Shower (at least before meetings).
6) Be grateful:
a. Be so grateful for being heard that you learn to live off the power of your own gratefulness. Do not request a living wage.
b. Honorarium payments might be stopped to avoid service users becoming ‘dependent.’ Don’t question if clinicians are dependent on their salaries, it’s different.
c. Payments affecting ESA? It’s your responsibility to know how the trust will pay you and whether it will result in compliance interviews and sanctions.
d. Accept with gratitude the realms of white A4 you are given to read before each meeting taking hours for which you receive no acknowledgement (let alone pay).
e. Be grateful because no other people paid as little as you do get to sit at the tables you have the privilege of sitting at (whilst being ignored and patronized).
7) Listen to the wisdom of the professionals. You should also expect them to ensure the next meeting date is set at a time they can all do but say, “Well we don’t all have to be there” if you can’t do it.
8) Don’t be offended if someone pats you on the head and gives you some tea and a biscuit. It is for their benefit, not yours.
9) Do not under any circumstances dare to read up about your subject, quote relevant literature, or ask why involvement in your organisation does not acknowledge the work of people with lived experience, or seek them out to lead projects. You will be replaced by someone who is closer to the ideal service user – suitably compliant and ensures the pesky service user tick box is filled.
10) Accept the privilege you are granted (for all the wrong reasons).
11) Put aside any expectation that structural inequalities between service users will be acknowledged or countered. E.g. do not request that meetings and training are held in wheelchair-accessible venues.
12) If you are not recovered enough to be socially acceptable, please ensure you conceal this in public.
13) If you are presenting at a professionals’ conference and you have scars, expect to be asked intrusive questions in public and do not tell the asker to fuck off. This is also called “being professional”.
14) For every comment you offer that challenges the status quo, balance this with something that reaffirms the mental health nurse hero narrative.
15) Be a white middle class woman OR pass as a white middle class woman – actual economic capital is optional. NB do not expect any sexism from other service users to be defused by professionals in the room.
16) Remember that when it suits we are all human and all experience distress and are the same. This is collaboration, we are equals. Until we are not. Then you are some kind of personality disordered subhuman who is not to be believed or trusted and will have no say in the decision making.
17) Be prepared for even the critical folk to view you through the lens of your label.
18) Smile and laugh at hostile insults related to your diagnosis just after you have disclosed it.
19) Don’t object to non-person-first language such as “self-harmers”, “BPDs” or “frequent flyers” – that is just your diagnosis talking.
20) You are welcome to get involved with trusts. But be aware they reserve the right to contact your clinician or check your notes to attempt disprove what you tell them.
21) Be prepared to be told at your next needs assessment that your social needs are all met because you sit on committees with real working people.
22) Expect the professional liberals you thought were ok to shuffle papers & look the other way when you call out their colleagues’ discrimination.
23) There’s opinion, clinical opinion and “just your opinion”. Please note that the gold standard of evidence does not include service user evidence and Randomised Controlled Trials rule.
24) Accept that no matter how many other SUs you have consulted with the views you bring will never be representative of all patients, but one clinician speaks for all clinicians.
25) Be prepared to dedicate all waking hours to try and make a difference only to still be treated with utter contempt in your own care. Don’t get frustrated, it’s probably your own fault. You are not working hard enough on your skillz.
26) People will be paid more to listen to your experiences of being traumatized by the system than you will ever be paid for sharing them. Deal with it.
27) Accept that your successes will be used as a stick to beat other service users with, while your weaknesses will become evidence that it is unwise to involve service users at all.
28) You may well find yourself in a position where you feel hated by clinicians for being challenging but also silently hate yourself for feeling like you have sold out.
29) As a service user you can never possibly understand the time and financial pressures of the NHS. If we tell you we need an expert by experience with a diagnosis of schizaloopia to attend a far-away village at 8am tomorrow morning having read a 40 page document and you think that’s unreasonable, it’s because you don’t understand. Be grateful we asked you.
30) Finally, remember: everything that hurts you is outside the trust’s / university’s control. Everything you like is down to their hard work and professionalism.
HAPPY CO-PRODUCTION WEEK!
This is covered by a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) License
Wow! What a day! Recovery in the Bin had their abstract accepted for a poster and short presentation at the Royal College of Occupational Therapists’ Conference in Belfast on the 12th of June 2018. We were very excited to be able to share our work at such a big and prestigious event.
This blog post is an opportunity to expand on our poster and presentation. It is also a resource for those who were unable to attend who may want to know a bit about us and our work. As it is for a wide range of audiences, we have included an Occupational Therapy Language Translator for those who are not familiar with the language used by occupational therapists – or maybe more appropriately – the way occupational therapists understand and use certain words : )
For in depth critiques on the notion of recovery, please feel free to browse the groups numerous blog posts.
To reference this blog please use the following:
Recovery in the Bin, Edwards, B. M., and E. Thomas (2018, June). Recovery in the Bin at #RCOT2018. Blog based on Facilitated Poster presented at the Royal College of Occupational Therapists’ Conference, Belfast, UK.
Occupational Therapy Language Translator!
Occupation:
Most people associate the word occupation with the words, job, career or vocation. Some associate it with the occupation of land by military force.
However, occupational therapists use the word occupation differently. In its broadest sense, the word occupation can refer to anything that somebody occupies their time doing – literally anything!
Occupational therapists typically split occupations into 3 main categories – Self-care, Work and Leisure. Work does not necessarily mean paid work – it can mean voluntary work and other things classed as work, for example house work, caregiving, DIY. Importantly, the definition should always be made by the person themselves – some people might think DIY is a leisure occupation etc…
What was the presentation about?
We decided that the Unrecovery Star would be a good introduction to the groups philosophy and views on recovery – it is visual, and it has a catchy name! Most importantly, we wanted to emphasise that our work is survivor and service user led, although we have members who are also health and social care professionals.
Why are Recovery in the Bin critical of recovery?
Everyone working in mental health services has heard of the word recovery. You cannot read a mental health policy without coming across the word on multiple occasions.
So what’s wrong with this? Isn’t recovery a good thing?
Unfortunately, since recovery has become mainstream and has been implemented across health and social care services, it no longer represents its original ethos that made it so popular.
It is no longer service user or survivor led, and it is no longer radical: Professionals typically lead or control the recovery process and the services in which a recovery approach is delivered.
Conversely, the notion of recovery originated from grassroots service user / survivor organisations, which placed emphasis on personal meaning and agency, in contrast to a traditional professional led approach.
The current power imbalance in service provision is incompatible with recovery’s origins.
The impact of Neoliberalism and Austerity
Recovery in the Bin is critical of the influence our socio-political environment (primarily neoliberalism and austerity) has had on recovery’s implementation, and peoples understanding of recovery. Recovery’s original emphasis on what is personally meaningful has evolved to reflect neoliberalism’s overemphasis on personal responsibility and choice.
Services and working practices have changed to reflect this. The premise that continued involvement or contact with services results in ‘dependency’ and a lack of ‘responsibility’ is widespread. Discharge is the goal, whether recovered or not.
Neoliberalism’s emphasis on personal responsibility and choice, fails to acknowledge the social injustices inherent in a neoliberal society that prevent choice and minimise others’ and societies responsibilities. Recovery in the Bin challenges neoliberalism’s individualism by advocating a collectivist approach. It highlights society’s role in addressing social injustice and creating a socio-political environment that enables a meaningful recovery.
What is the Unrecovery star?
The Unrecovery Star was developed through consensus based and participatory methods by Recovery in the Bin. It visually depicts the socio-political barriers faced by people living with mental health conditions or distress, which inhibit recovery. As such, it directly contrasts the individualised focus of the traditional ‘Recovery Star’: The Unrecovery Star does not place the responsibility and burden for recovery on the individual, rather, it situates recovery within the wider context of social change.
It is not a validated outcome tool. Instead, its purpose is to encourage clinicians to become aware of the way the recovery approach is implemented in practice, with an over emphasis on the individual as opposed to society. It promotes critical reflection on the recovery approach from a socio-political perspective. It seeks to strengthen clinicians’ commitment to social justice
What implications does it have for occupational therapy?
Holistic Practice:
Occupational Therapy Language Translator!
Holistic:
Occupational therapists use this word a lot. It means that they look at the whole person, not just the ‘condition’ or difficulties a person may experience. This includes their environment – physical, social etc, what’s important and meaningful to them – their values, their interests, their habits, what they enjoy doing and how they think and feel about themselves.
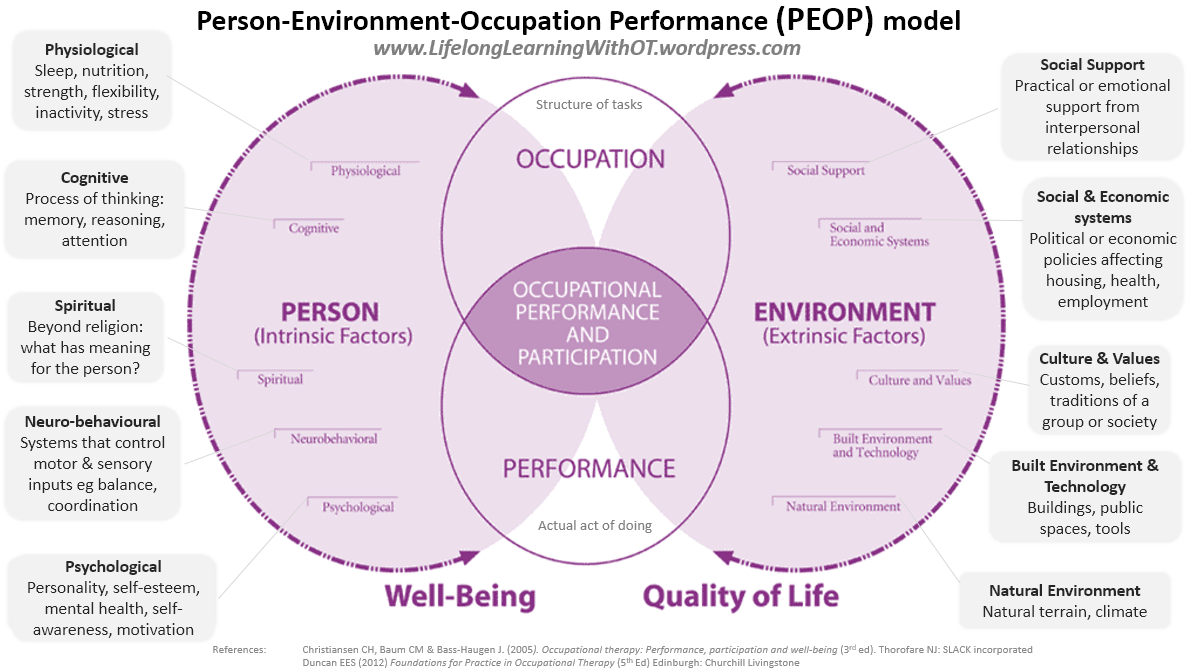
As this blog was produced at short notice – this section will be updated to include examples of holistic practice! Here’s an OT model of practice, which gives you an overview of what we mean by ‘holistic’. This model does outline ‘Social and Economic Systems’ well.
As a holistic profession, occupational therapy purports the dynamic interaction between a person, their occupations and their environment (Taylor 2017).
As a tool to aid critical reflection, the Unrecovery Star can be used to enhance holistic practice by increasing occupational therapists’ awareness of the socio-political environment and its impact on occupational participation and recovery.
This could include welfare reform, for example, the Bedroom Tax, cuts to Employment and Support Allowance and DLA / PIP, which may limit the amount of money someone may have to access and participate in meaningful occupations. Cuts to local government funding have meant that many local libraries have shut, and community groups have ceased to exist. This restricts people’s occupational opportunities and the freedom people have to make occupational choices. Packages of care are being restricted and so are programmes of intervention. Recurrent ESA and PIP assessments may have an on-going long-term impact on someone’s occupational identity as a person: emphasis on work and productivity can diminish the value people believe they have as occupational beings.
These broader aspects of the socio-political environment can and often remain hidden. Standardised assessments may not be particularly attuned to picking up these wider, insidious influences on occupational performance. Critically reflecting on the recovery star can facilitate this insight which can be used during the assessment process to inform realistic plans of intervention. In addition, it can aid critical reflection on the service and organisational environment within which occupational therapists work. In particular, this could include the socio-political environments’ impact on the way the recovery approach is implemented locally.
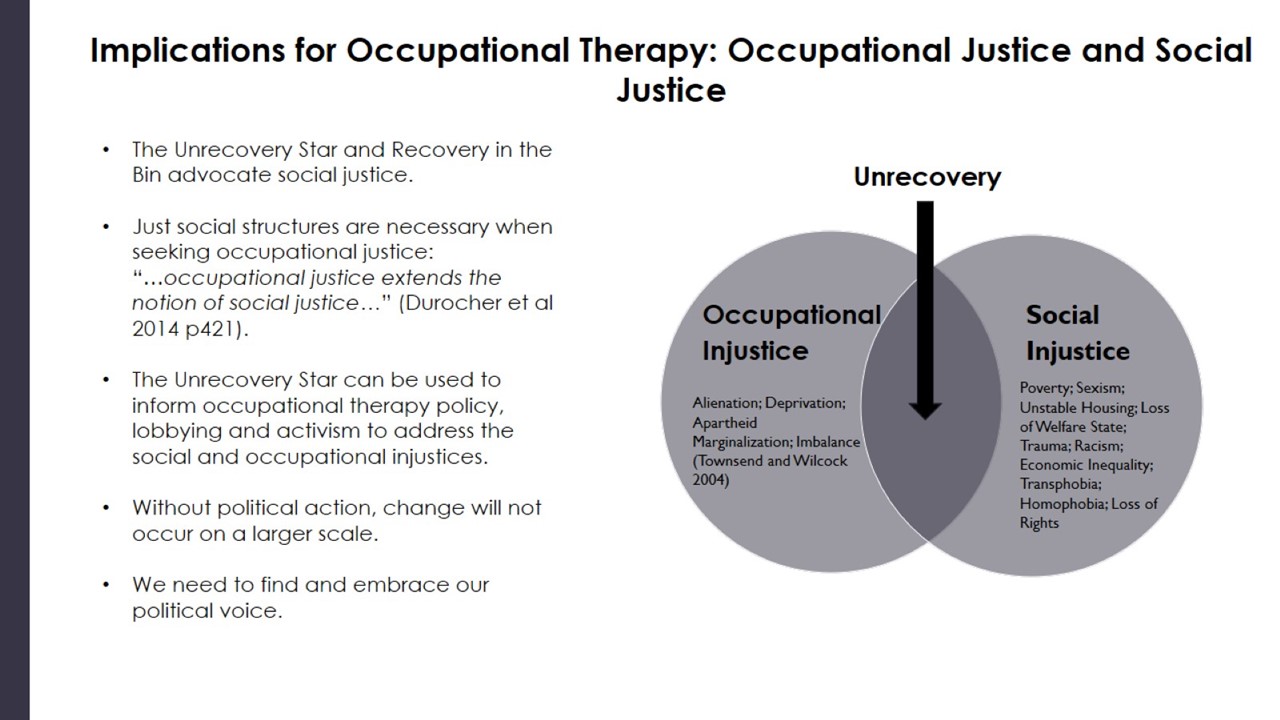
2. Occupational Justice:
The Unrecovery Star’s emphasis on social justice closely aligns with the notion of occupational justice. As Durocher et al (2014) states, “occupational justice extends the notion of social justice” (p421): Just social structures are necessary when seeking occupational justice. The Unrecovery star raises awareness of the particular social injustices people with mental health conditions experience, which must be addressed when seeking occupational justice.
Both occupational and social justice call for political action. Given the socio-political injustices, including austerity and welfare reform, that people with mental health conditions and distress experience, it is time to find and embrace a political voice. As a profession, occupational therapists can bring these injustices to the attention of decision makers and governments through policy, lobbying, activism, petitions and protest.
Without political action, occupational and social injustices cannot be changed on a large scale.
Post Presentation Questions (not word for word…relying on poor memory!):
Unrecovery can come across as quite a negative word. How would you respond to this challenge?
That’s a great question. Unrecovery should be seen as the same kind of ethos as ‘unconference’ or ‘antiuniversity’*. It’s about including the excluded, going back to the grassroots. Surprisingly, Recovery in the Bin is not actually opposed to ‘recovery’. What we want to bin Is the ‘Recovery Approach’ in the form it often takes in services that can be very far from Recovery’s original values: commitment to the service user and personal meaning.
*Unconference can be described as participant-driven meetings that try to avoid top down organisation, fees, sponsorship typical of conventional conferences. Antiuniversity is about free and inclusive learning events and as such challenges academic and class hierarchy that may exclude people who aren’t privileged in society.
How can Recovery in the Bin’s materials be used in a Recovery College?
The Unrecovery Star could be used to discuss Recovery’s original values and give service users the opportunity to talk about how it may be being implemented in services. Perhaps it could be shared with participants as part of discussion about how to challenge professionals or colleagues or managers who may be implementing recovery in a way that departs from the original values of recovery. It could also be used to think about how society’s responsibilities and duties toward people influence an individuals recovery and personal values, goals and meaning^
^We also have a blog on Recovery Colleges. This hard hitting satire was meant to challenge. It had a very positive impact resulting in an editorial in a per reviewed journal, by the founders of Recovery College’s focusing on how colleges could return to their original principles when they drifted into the kind of practices satirised by RITB’s ‘Stepford Recovery College’ blog.
The United Nation’s Committee on the Rights of Persons with Disabilities Report.
Living independently and being included in the community (art. 19)
44.The Committee is concerned about:
(a)The fact that the State party’s legislation fails to recognize living independently and being included in the community as a human right that enshrines individual autonomy, control and choice as intrinsic aspects of that right;
(b)Policies and measures that affect the ability to live independently in the community, such as the reduction in social protection schemes related to housing, household income and budgets for independent living, as well as the closure of the Independent Living Fund;
(c)The fact that responsibility for supporting independent living has been transferred to the devolved administrations and local authorities without providing appropriate and earmarked budget allocation;
(d)The fact that many persons with disabilities are still institutionalized and deprived of the right to live independently and be included within the community, when: (i) they lack the financial resources to afford personal assistance; (ii) local authorities are of the opinion that they can provide assistance within care homes; and (iii) the cost rationale constitutes the main parameter of an assessment;
(e)The lack of support services and accessible public facilities, including personal assistance, for persons with disabilities, regardless of sex, gender, age and other status, to live independently and be included in the community.
The Committee recommends that the State party, in line with the Committee ’ s general comment No. 5 (2017) on living independently and being included in the community and the Committee ’ s report on its inquiry concerning the United Kingdom of Great Britain and Northern Ireland carried out under article 6 of the Optional Protocol to the Convention:
(a) Recognize the right to living independently and being included in the community as a subjective right, recognize the enforceability of all its elements, and adopt rights-based policies, regulations and guidelines to ensure implementation;
(b) Conduct periodic assessments in close consultation with organizations of persons with disabilities to address and prevent the negative effects of policy reforms through sufficiently funded and appropriate strategies in the area of social support and living independently;
(c) Provide adequate, sufficient earmarked funding to local authorities and administrations, including the devolved governments, to be able to continuously allocate adequate resources allowing persons with disabilities to live independently and be included in the community and to exercise their right to choose their place of residence and where and with whom to live;
(d) Set up a comprehensive plan, developed in close collaboration with organizations of persons with disabilities, aimed at the deinstitutionalization of persons with disabilities, and develop community-based independent living schemes through a holistic and cross-cutting approach, including education, childcare, transport, housing, employment and social security;
(e) Allocate sufficient resources to ensure that support services are available, accessible, affordable, acceptable, adaptable and are sensitive to different living conditions for all persons with disabilities in urban and rural areas.
These are the slides from the Recovery In The Bin presentation to the Royal College of Occupational Therapists [12/06/2018] PDF HERE > RCOT Presentation RITB
To reference these slides please use the following reference:
Recovery in the Bin, Edwards, B. M., and E. Thomas (2018, June). The Unrecovery Star: A survivor led critical discourse on the notion of recovery in mental health. Facilitated poster, presented at the Royal College of Occupational Therapists’ Conference, Belfast, UK.
This is covered by a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) License
Psychotherapist Paul Atkinson talks to Richard House about being a mental well-being activist and the daily difficulties faced by those on the therapeutic front line
Richard House [RH]: Paul, activism takes many forms – including ‘psy activism’ (my term) in the realm of mental health; and you’re one of the most committed psy activists I know. Can you say something, first, about what you see as the key commitments of a psy activist who also works professionally in the mental health field?
Paul Atkinson [PA]: For me as a psychotherapist, the key commitment is an ongoing awareness of the inevitable and complex power relationship between psy professionals and clients/service users. This applies to activism, and also to the consulting room itself. Psy professionals often claim an apolitical neutrality and an enhanced empathic sensitivity in their relationships with other people. Unless we’re willing to continually pay attention to the limits of our assumptions and experience, and keep learning from the people we’re working with, we’re likely to be projecting subtle, and not-so-subtle messages of knowing more than we know, of being a little (or a lot) more important than we are, and protecting ourselves with a whiff of authority that’s overbearing or condescending.
One of the particular characteristics of mental health politics, of course, is that what we call “mental ill-health” is very likely to be a response to the abuse or misuse of others’ power over us at different periods and settings in our lives. So the fact that so much service mental health provision is top-down – in the form of the politics of commissioning and funding, as well as the diagnostic and treatment decisions of psy professionals – is a fundamental issue for mental health activism. As far as possible, political activism around mental health must be shaped and led by service users and survivors. For psy professionals, trust can only be earned over time through action, alongside and in support of survivors. Obviously we professionals have plenty of political issues within our own working remits, around which we can take the lead. But we’re so much more powerful in our campaigns if we have allies campaigning with us who are on the receiving end of the dysfunctionality of the psy professions.
RH: There’s a lot there, Paul! Can you tell us how far away current mental health provision is from the “bottom-up” approach you’re advocating here? – and whether you think a radical-left government could really make a difference to that – and if so, how? magine Iyou’re the new minister for mental health and you have five years!…
PA: I think there are fantastic examples of grass-roots activity among service users. I’m thinking of people I’ve met from the Mental Health Resistance Network, Disabled People Against Cuts (DPAC – regularly featured in the Star, of course), Recovery in the Bin, Friends of East London Loonies, the National Survivor User Network, Kindred Minds, the Survivor Researcher Network and Making Waves, as well as hundreds of small user, refuser and survivor-run groups involved in peer support, political campaigning, the creative arts, in manifold ways of sharing and valuing each other’s lived experience. But the culture-gap that exists between these forms of local “activism” and mainstream top-down mental health services provided by the NHS, or by some of the big mental health charities like MIND, can be enormous, and often very toxic for people suffering psychological distress.
Do I think a radical-left government could really make a difference? The political transformation required to rethink mental ill-health as a function of society’s ill-health is profound. In a way, mental-health politics is at the heart of any real questioning of what kind of society we want to live in, how we want to relate and be related to, what and whom society’s for. The first three jobs of a radical minister for mental health should be: (1) To ask user groups and individuals all over the country what “mental illness” means to them, and what would be of help to them. Mean it, listen, and then carry on listening. If the Labour Party were serious about any kind of radical transformation of mental health policy, it should be doing this right now. Are they?… (2) Give people the material resources to support their basic needs without condition. (3) Ban all forms of coercion in the name of “treating” people’s psychological suffering/distress.
RH: That’s a resoundingly clear statement – and challenge – to Labour’s shadow health team, Paul: let’s hope they’re open to listening, both to your conspectus here and to the experience of those who desperately need to be listened to – and who, to date, rarely have been by the Establishment. I really like how you place your emphasis on political receptivity and user empowerment, rather than on top-down initiative-itis. I assume you’re less than impressed by current state therapy provision and its top-down nature?
PA: Well, NHS primary care therapy provision – Improving Access to Psychological Therapies (or IAPT) – is seriously top-down. It’s organised as a sort of factory-system or conveyor-belt of mental health treatment, offering on average six or so sessions of cognitive behavioural therapy (CBT), or perhaps mindfulness, relaxation, or online self-guided exercises – aimed really at getting people suffering from depression and/or anxiety back into the everyday reality of their lives under capitalism. What kind of therapy you get is decided for you through a diagnostic check-box interview which may be held on the phone, or even by computer. There’s very little room for “user choice”. Out of 1.4 million people referred last year, two-thirds either never entered or failed to finish a course of IAPT treatment. They simply disappear from the statistics. I’m afraid it’s hard not to feel that IAPT is more about providing cover for the mental ill-health of capitalism than it is responding to the psychological suffering of the people.
Beyond IAPT, I think all forms of therapy carry the danger of encouraging a way of thinking about one’s self and the world that’s imposed on clients, rather than evolving through a process of mutual exchange between a therapist and a client.
RH: That’s sobering stuff, Paul; but I suppose we shouldn’t be too surprised when (state) capitalism creates a form of therapy that’s cast in its own image. Finally, could you say something about the once-again mooted state regulation of the psy therapies, and why you think this would be harmful to the field and to the work of therapy?
PA: Obviously therapists want their work with clients to be accountable. The problem with state regulation is the state’s desire for psychotherapy. As we see in other fields like education, medicine, and the law, the neoliberal state is increasingly engaged in violently undermining and taking political control of professional practice whose values and traditions conflict with the interests of the market. Psychotherapy, especially in the independent sector, operates at its best as a sort of free association and open exploration of meaning between people, a process that fosters possibilities for individual and social transformation. In the hands of the state, it will gradually and inevitably be reduced into the service of market agendas.
Paul Atkinson is a psychotherapist in independent practice in London, and a member of the Free Psychotherapy Network. Richard House is a Corbynista activist living in Stroud.
One of the responsibilities of doctors (leading to great privilege in the form of good wages and social status) is to act as an informed, accurate and unbiased opinion about people’s access to welfare on the grounds of health problems. Another responsibility of the doctor is to act as an advocate for their patients so that they can access welfare they are entitled to by any reasonable interpretation of the requirements as well as to protect them from any adverse effects of the welfare system that they are vulnerable to. This responsibility can be discharged by communicating with the relevant welfare agencies by various means such as filling out forms, writing letters and direct communications by phone or email. In this blog I tend to use the term “patients” as a generic term used for people consulting a doctor.
Whilst the social model of “disability” is by far the most helpful in order to plan interventions to reduce adverse consequences of mental health problems (my crude understanding of this model is what barriers are there that prevent this person’s desired participation in society including access to their needs for food, shelter and security being met), access to benefits are based on a more medical model of medical condition (identified by diagnosis), associated impairments in functioning and resultant disability (lack of capability or restriction) and social disabling (subsequent disadvantage and lack of fulfilment of social roles such as work or independence without care).
A first point is that the diagnosis is usually insufficient and details need to be given about any resultant impairment. For many diagnostic constructs, the diagnostic criteria are used to identify the best-fitting diagnosis and are not in themselves the whole nature of the condition. To use a general medical example, myocardial infarctions (“heart attacks”) are often identified using a combination of cardiac muscle enzyme results, ECGs, typical descriptions of symptoms and so on but the myocardial infarction itself is a blockage in the blood supply to the heart muscle leading to death of cardiac muscle tissue and resultant complications. It is this blockage and resultant complications that leads to death and impairment in functioning but the diagnostic criteria are used to identify the condition and access to correct treatments and as a first step to other help such as benefits if unable to work afterwards.
Depression is more than just the listing of diagnostic criteria in diagnostic manuals (and in this case the criteria are not as clearly linked to an underlying cause as they are for myocardial infarction). It is this whole nature of depression that is important for the purposes of access to benefits – lethargy, the dread of any change in case it makes things worse, the loss of confidence, the self-doubt, anxiety, avoidance of social contact, poor concentration, thoughts of self-harm etc. The diagnostic construct means the person is more likely to have features associated with that construct that may make them eligible for benefits. It is then up to the doctor to spell out what these features are, what treatment they are receiving, whether they are receiving services such as inpatient or day patient or outpatient, what impairments in functioning result and/or what risks arise to the person or others and what nature of support is needed from others. For example, if someone has agoraphobia they will struggle to leave the house – one consequence is they will find it hard to keep a job. Someone with dementia may wander and get lost so need somebody supervising them. Somebody who is suicidal is a risk of death so will need support and watchful care.
There several papers I use to help me fill out these forms (see references, all open access but all last millennium) but care coordinators such as CPNs and social workers are much more aware of the intricacies and requirements of the system. CAB and welfare rights organisations can provide helpful guides to completing form.
The second point and one frequently made is that the benefits system suits physical health conditions better. It is much harder in mental health to demonstrate that the impairment in functioning is due to the condition – for the myocardial infarction there are tests both associated with diagnosing the condition as well as associated impairments in functioning. In mental health apart from some exemptions such as dementia the demonstration of impairment in functioning is often reliant on the “word” of a mental health professional – it is therefore necessary to fill in the forms requested by benefits agencies so that the doctor’s patient can prove their eligibility. The benefits agencies will weigh up the reports of impairments in functioning, the risks and need for support and care.
The third point is that the benefits system can cause distress to people who are most vulnerable to this problems and increase their mental health problems and risks. Waiting for benefits with no income or savings leads to practical problems as lack of access to food and how to pay the rent multiplied many-fold if the patient has dependents like children. Assessments including reviews of eligibility are major existential threats to many patients on benefits. The lack of tests in mental health mean patients fear they will be disbelieved and the stress caused by these procedures can lead to relapses of mental health conditions and increased risks such as suicide. It is important that mental health services support their patients by completing these forms and if necessary direct contact with benefits agencies – by phone, letter or email – to point out these adverse and counter-productive effects so that patients are protected from these effects.
It is the duty of doctors to help their patients access benefits to which they are eligible, to provide accurate unbiased information as needed to benefits agencies and to help patients by interceding if they are suffering adverse effects from the procedures of the benefits agencies.