Dear Mad in the UK and the British Psychological Society, We are writing in regards to the article ‘Prescribing Rights for UK Psychologists – Should We Be Cautious?’, written by prominent psychologists who are members of the British Psychological Society. Whilst we recognise that prescribing rights for psychologists is a complex issue, we are contacting you specifically about a passage in the article that appears to express transphobic views.
We refer to the following passage, which we also note is the only section without any references, suggesting strongly this is a work of personal opinion by the authors:
‘Gender services The prescription of hormone blockers for people who identify as transgender is a highly controversial trend, raising profound issues, both conceptual (about the validity of a diagnostic category of ‘gender dysphoria’; about the relationship between biological sex and gender roles, and so on) and ethical (the long-term effects of these drugs is untested and unknown). We do not believe that prescribing rights should be extended to psychologists working in these areas unless and until these wider issues achieve some degree of resolution and consensus.’
Hormone blockers are a legitimate and common treatment for those who are transitioning to their identified gender. It is unclear why the authors view hormone blockers as ‘controversial’ or a ‘trend’. No references are provided to support the use of these words. Both words are value loaded, and on reading, appear to undermine the legitimacy of the process of transitioning with hormone blockers to one’s gender identity. It should be noted that taking hormone blockers does not by itself imply an irrevocable commitment to transition, but merely leaves open the option to do so with less dysphoria and potentially less exposure to societal prejudice. Undermining and describing the process of transitioning as ‘controversial’ and a ‘trend’ is transphobic.
We also note that the passage refers to the ‘profound issues’ ‘about the relationship between biological sex and gender roles etc’, again without references to support these statements. We note that the authors use the phrase ‘gender roles’ rather than ‘gender identity’, however, we read this as a veiled statement referring to the opposition by some to the very idea of transitioning, emphasizing biological determinism over trans people’s lived experience as a different gender to that they were assigned at birth. This is a transphobic view, and by including these controversies in their article, the authors legitimise these views.
To provide a context to our concerns, please see the current Stonewall definition of transphobia: The fear or dislike of someone based on the fact they are trans, including the denial/refusal to accept their gender identity.
We are therefore, writing to you as publisher (Mad in the UK) and professional body (British Psychological Society) to request that you investigate these statements. We would also like to highlight that this is not the first time some of the authors have expressed transphobic sentiments.
Signed
Recovery In The Bin Manchester Disabled People Against Cuts The London Bi Pandas Mental Health Under Capitalism Leeds Sisters Uncut
Service User Research Enterprise (SURE) team: Diana Rose Stan Papoulias Akriti Mehta Ruth Silverleaf
Alison Faulkner Jayasree Kalathil Len Demetriou
CliniQ CIC Michelle Ross (founder cliniQ CIC) Vincent Turner (psychotherapy lead cliniQ CIC) Martha Dunkley (director cliniQ CIC)
National Union of Students Piers Wilkinson, NUS Disabled Students’ Officer Eden Ladley, NUS Trans Officer Rachel Watters, NUS Women’s Officer Liam McCabe, NUS Scotland President Robert Murtagh, NUS-USI President
Daira Hopwood Shabaaz Mohammed Dennis Queen Mx J.M. Welch Dr Sally Morgan, Clinical Psychologist Ms Sali Owen, LGBT+ Group Facilitator for Forensic In-Patients Sally-Anne Beverly (University of Leeds) Sue Sibbald Dr Joanne Edge, survivor Robin Edwards, Notts Trans Hub Stephanie Allan Sue Phillips Josephine Sirotkin Edie Boon Dr Aylwyn Walsh, Associate Professor, University of Leeds Clare Bonetree Dr Alexandra Richards, Clinical Psychologist Rachel Rowan Olive, service user / survivor Karen Pollock GRSD specialist counsellor Dominic Davies, Pink Therapy Jamie Draper Sam Hope, MBACP (Accred.) Neil Loffhagen GSRD therapist / counsellor Esther Kaner Nāgakuśala Frugal Sam Feeney, Dip Coun, Dip Gender/Sexual Diversity, Reg. MBACP Dr Mari Greenfield Ronete Cohen, GSRD Psychotherapist, The Rainbow Couch Debbie Helen Wood, trans and talking therapies lead with Outreach Cumbria Rachel Yates, Counsellor Jules Haley, GSRD Therapist / Counsellor Hannah Ryan, Trainee Clinical Psychologist Gary, patient and activist Tony Roberts, Director, Fostering Change Ltd. North Yorkshire Charlie Rodgers Lorna McArdle, Support U Alyssa Henley, Support U Zoe Ereni, writer, training psychotherapist Debra Shulkes
If you wish to add you or your organisation’s signature to the open letter please email recoveryinthebin@gmail.com
Workplaces blame or punish individuals for madness, exclude mad people from work, and fail to recognise the role of work in making people mad in the first place. This is true even of measures supposedly designed to enable accessibility or promote mental health. Sick of this, I asked some members of radical and peer-led mental health groups, along with some friends and fellow weirdos, what they think would make it better to be ‘mad at work’. I collected all the responses, merging duplicates and re-writing stories into demands, to make the list below.
Of course one of the best things workplaces could do for mad people would be to improve their economic conditions. Many folk brought up precarious employment as especially harmful, including short-term and zero-hour contracts, as well as people having to re-apply for or apply for funding for their own job. As long as there is capitalism there will be suffering for mad people at work, exclusion of mad people from work, and madness as a result of work. Although this list is not primarily about economic conditions, is not intended to justify wage labour or erase the harm it causes.
Yet many of the suggestions made below are perfectly compatible with the logics of capitalism. Some mad people just want to get through the day however they can. They want to have a nap sometimes, dress more comfortably, mask less, not get lied to and – perhaps most of all – be subject to less surveillance. These things are cheap, straightforward, and would even enable mad people to ‘more productive’ workers within the grim logics of capitalism. So why are most items on our list still completely unimaginable?
OUR DEMANDS
No glass walls or doors for maximum privacy and minimum surveillance
All toilets to be accessible and all-gender
Provision of private nap cubicles
Abolition of gaps around toilet doors to allow for privacy for purging and panic attacks
Provision of luxury harm reduction rooms, including beautiful soft furnishings, safety equipment (wipes, clean needles and razors, sharps bins), and gold boxes for everyone to keep their individual stuff in
No dress codes or norm of dressing gowns, blankets, pyjamas, slippers, bare feet
No more defining mental health as the ability to work
Abolition of counselling as gatekeeping for jobs
End of the use of health and safety and risk assessments to punish and restrict autonomy of disabled people
Abolition of small talk (replace with standard red/yellow/green communication badges every door)
Police uniforms for Human Resources & Occupational Health staff to make their roles clear
Paid time in all workload models for collective organising (including but not limited to trade unionism, direct action, feminist consciousness raising and zine-making)
Free workers’ canteens (with no coercive ‘health’ or ‘normal’ eating)
All contracts mandatorily available as job share
All workplaces to circulate and commit to Recovery in the Bin principles
Worker feedback forms to be located over the shredder for clarity around purpose
No more macho pretend-its-fine culture
Actually flexible working hours
Recognition of workers as humans for whom work is only one part of life
Abolition of workplace communication by whatsapp, ‘fun’ group chats that include bosses and all social media (except personal or political social media use at work)
Time in all workload models for private, skilled, on-demand clinical supervision for anyone who works with ‘vulnerable’ groups
Recognition that learning, not-knowing and lack of enjoyment are inevitable elements of work and not signs of unprofessionalism
Resources to support working from home (e.g. printer and scanner)
Option to get paid based on hours or on task, your choice, with no reduction in pay (maximum 25 hour work week either way)
A sensory room with sensory toys AND integration of those things into rest of work place
No forced disclosure ever
Sound proofed screaming cubicles
Screaming normalised everywhere, ear defenders supplied at all entrances
Employers to pay employees’ union membership
No more suffering as a rite of passage
Education for all employees about madness BY mad people
Abolition of the idea of ‘professionalism’ (otherwise known as ableism, racism, misogyny, etc)
Abolition of ‘reasonable adjustments’, replacement with actually accessible workplaces including accessibility budget for all workers with no monitoring
Wages for housework, care labour and all social reproduction
No more rest or breastfeeding areas in stationary cupboards
Repurposing of ‘common room’s for crafting, animal therapy, prayer, dart boards and punch bags with bosses faces on, meditation, etc.
No more token wellness activities or ‘pledges’
More sharing of unsantized stories (NOT ‘it all got a bit tricky but I’m totally better and promotable now’)
Abolition of requirement to perform trauma and healing for job
No more blaming our mental health for impossible working conditions
By Darcy Leigh.
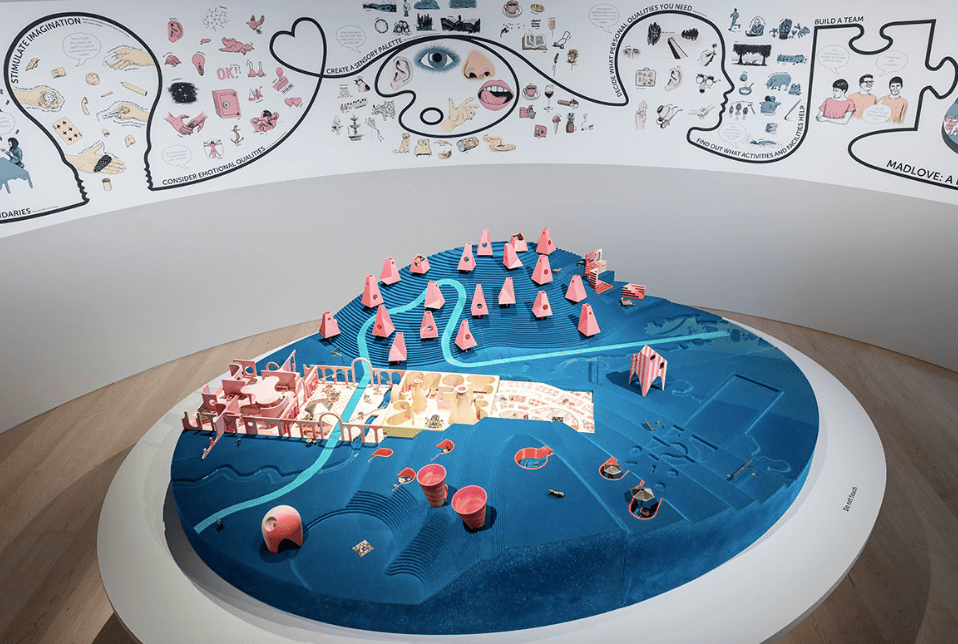
The making of this list was inspired by the Mad Love Designer Asylum project, in which mad people design their own asylum.
The following is a preamble for Blog as a memoir of sorts – not a rant – to hopefully go towards improving things for BAME survivors (victims?) of psychiatric torture…and to also, hopefully, help to prevent atrocities of this nature from being so free to occur in times future for others.
Racism in the Bin !
I thought it would be useful to start by writing about my own years long ordeal…and I would advise others not to share their stories at this stage in the game or to comment either using your real name…fear of reprisal and/or guilt by association is well founded/understood.
I am informed and aware enough (I think) that there are some good psychiatrists out there but unfortunately we cannot assume that they have enough humility, autonomy or freedom from the herd/autocracy/hierarchical forces to not otherwise be what I call ‘psychiaracists’ such as the ones who said to me years ago :”you do know that you have a black gene, don’t you, which is causing you to be mentally ill”…Glory!
Whatever a person’s colour or tribe might be this doesn’t automatically stop him/her from subjecting a person to ‘cruel and unusual punishment’…the so called nurses who physically tortured me were/are also ‘black’…
My ‘psychiatrist – elect’ is a Jungian analyst. Carl Jung was a Swiss psychiatrist and founder of analytical psychology. Jungian analysis isn’t so accessible unless a person pays privately here in the UK. His opus or great work was/is dismissed by so called normal people who put so much store by ICDeologyconformity/mediocrity/ignorance (?).
Furthermore, I was very surprised to hear that the consultant psychiatrist who diagnosed me as Bipolar when I was about 39 years old hadn’t even heard of Jung – the same psychiatrist who said that I ‘have a different kind of brain’ which according to him ‘lacks the foundations of an ordinary building’…whatever next ?
“Show me a sane man and I’ll cure him for you” – Carl Jung 🙂
No one knows everything there is to know about the mind – fortunately ! – just as no one can predict the future in life. Jung was a gnostic – didn’t fight shy of the ‘mystical element’ …and his writing – as with anyone else’s – has to be seen/evaluated fairly with respect to time of writing and so on…
He was slated by the herd recently enough, too, for being racist…my late former Jungian analyst who was a Jewish woman said he was not ‘racist’ – that he was exploring the collective unconscious, the shadow and his own. Jungian analysts have to know themselves – including deeply understanding prejudices, projections and dark side or shadow – very well before and as part of being/becoming an analyst. I have sampled other schools of psychotherapy/psychoanalysis and found the Jungian school suited me best – not because I am a racialised human being…more to do with having such an expanded consciousness – propensity for ‘manic phases’ – and/or my falling into the unconscious and the ‘numinous’ or ‘mystical’ realm, even, which was initially triggered by my drink being spiked unawares with an hallucinogenic drug at a party many years ago. I also read quite a lot of his writing in my early twenties…beginning with his autobiography titled: “Memories, Dreams and Reflections”…
There would appear to be little or no room for the ‘mystical element’ here in the UK..ICDeology is so reductive – limited/limiting, isn’t it?
“All thought is limited” – Jiddu Krishnamurti
I experienced ‘flashbacks’ which can look like hypomania but is not the same thing…it would appear that drug -induced psychosis and the damage to /impact on the brain of this isn’t actually very well understood. It’s highly dishonest to claim that an hallucinogenic drug triggers an underlying condition…this writer was ‘normal’ or ‘neurotypical’ enough beforehand.
My current analyst has a different approach…he recommended reading “The Drama of the Gifted Child” by Alice Miller…and has helped/helps me to see and understand enough to confront the cruel and unusual position I have found myself in…he said that therapy is about feelings. And. yes, unlike state – funded biomedical psychiatrists whose preoccupation is about control and limitation, really, he gave me a tissue for my tears…instead of dismissing my feelings as ‘lability’ and a reason or excuse to give me even more drugs.
“There’s a fine line between genius and madness”
Psychiaracists don’t acknowledge a person’s intelligence…or care about it either and hence the disproportionate labelling and over-medicating of black folk…a self-fulfilling prophecy perhaps ? Not possible to be or sound intelligent when a person has had a chemical lobotomy !’They’ have also inherited a shared delusion that ‘black’ people are dangerous as y’all know already I’m sure…when I recover the ability to act or appear dumb enough in a chemical straitjacket they’re happy to discharge me. Actually, this isn’t quite so since what typically happened was that they visited a section – legally or otherwise – on me for 6 months and then would discharge me just before the tribunal hearing date …in order to avoid the hearing no doubt.
The one and only tribunal hearing I have had in 20 years – a few years ago – I won…and against the odds if a person was to believe what is written in my psych notes… White female Judge; “Are you saying that although Katy who is now in her mid fifties – has no criminal record and clearly respects the law – is a danger to others?”
Black male psychiatrist: “Yes”
I hope that I never lose the ability to cry – respond to sorrow and to care deeply about people and all the needless suffering arising from and caused by the psychiatric system in particular- even though my tears have been labelled and dismissed /diagnosed as ‘lability’ – where’s the humanity/compassion in that ?
Some of the cruel and dishonest things the psychiatrist said about me at the tribunal even though he’d only just met me made me cry. He then said : “Look, see – she is labile !”
More to say about this encounter/travesty …later…
My analyst said that he knows how dangerous it is for me to feel things…and yes it is such – I am a psychiatric torture survivor after all. I am not ‘free’…apart from being free to be a virtual recluse – free from the ‘usual reign’ as TS Eliot would put it at this great age…
Freedom of expression and/or speech is not a given or honoured as a human right – especially if a person is psychiatrised and/or happens to be from a racialised group – is a black or grey (mixed race) woman with no ‘tribe’ to protect and support her like this nobody-writer…and/or who like me has/had a ‘precocious intellect’ – I was a gifted child…I am not a precocious person though – attitudinally-speaking…am ‘little-headed’ /self-effacing (usually)…very good at humouring people who have/had the power to torture me and decide my fate. However, my grey matter and ability to think critically has been extinguished more or less by all those needless chemical lobotomies and prolonged hospital admissions though now…and all for what ?
“It’s you my love you who are the stranger” – Leonard Cohen
My psych notes made for dark and humiliating reading…and opened my eyes…misrepresenting and demeaning a person in writing is always deliberate. As is/was totally covering up the one and only planned serious suicide attempt on my part during those ‘torture years’- (1998 – 2014) – Not only did they omit it from the notes they didn’t write anything about the reason for my trying to take a fatal overdose either…! The reason/cause being that I didn’t think I could/would ever be free from the haunting/damage of being subjected to total deprivation/solitary confinement (in 2012)…(or free from the fear of further torture given what took place the following year ).. A policeman in the hospital said quite angrily that “Katy is not the problem – the hospital is the problem!”
What a cruel thing to do to a person who started to break down – couldn’t sleep for a number of days – a few months after losing her mother who died very suddenly…I was in that terrible seclusion room just terrified for so long that I lost track of time and hallucinated* for the first time which is a common reaction to this form of torture – it also triggered suicidal feelings and caused me to lose the abilty to connect with and/or recognise others… The psychiatrist worried that she couldn’t ‘bring me back’ and thought I would have to go into a care home…she also changed my diagnosis which I have since rebutted. There were/are many other forms (of torture) which I have been subjected to as an inpatient – ‘behind closed doors’ – which I will write further about later…
As my solicitor said to me years ago :”unlike most people , Katy, the cure for you has always been worse than the complaint”…and then …an inevitable/inescapable revolving door scenario…a person who cannot escape physically can only do so mentally at the end of the day – living in constant fear of a hospital of all places is/was no mean chalk…needing asylum from the asylum now ain’t that absurd !
I used to also have laughter in me too – was not short of a sense of humour…the joke is on me though or so it would appear. (Laughing is perceived as being high for a person who has been diagnosed as Bipolar).
As a worker in what was a kind of unofficial Soteria house or ‘retirement home’ for people who’d survived God knows what in the back wards in Friern Barnet hospital, I /we argued the toss with the survivors’ psychiatrists; questioning the usefulness of medication per se whilst respecting the right on an individual level of the people living there to take medication if they did or did not wish to do so – of course, people need(ed) the right attention and care in life – not just drugs.. .
I was naive about my being ‘tokenised’ essentially or ultimately by a local Mind group which was at the time the most ‘politicised’ arm of National Mind – mostly and openly ‘anti-psychiatry’ and committed, too, to SU involvement as a must…
How could I know that this good work would/could cause me to suffer so greatly later on as an inpatient myself? The house was the first place of its kind and served as a pilot for others…(before the Care in the Community Act)
In 1998 I broke down following a huge bereavement…before being transferred from a good hospital to Satan’s Inn (anagram of Saint Ann’s) where I was repeatedly physically tortured by the male so called nurses, a woman who worked in the Mind advocacy office in the good hospital said she had a note about me which said : “we have to look after this one”…but they didn’t or perhaps couldn’t when I was transferred. I had never before had to enlist a solicitor’s help to get out of what was supposed to be a hospital!
Taking a break from writing now…Thanks for reading, Katy
I’ll write further about what I mean by ‘hallucinated’ later on perhaps… (Whilst it is not necessary or possible to include everything, some elements – especially those which illustrate the extent of iatrogenic injury – do deserve/need highlighting )
My admission was probably one of the lowest points at this time, I was pulled into an ambulance, by police officers who obviously had no idea how to handle a psychotic person. I was put in a small room with only my boyfriend there, three psychiatrists/psychologists came in and assessed me, I don’t remember much of the conversation apart from when one of them told me my parents didn’t want me and couldn’t take care of me. I was to be sectioned over the weekend. The first night I wandered around the ward crying, begging every nurse or doctor I could see for a second opinion. I just wanted to go home.
They gave me Lorazepam to keep me quiet and I didn’t sleep at all, I was on 1 on 1 for the first two days which meant I couldn’t be on my own, not to sleep, not to go to the bathroom or shower, not to cry or express the emotions I wanted to express. I felt helpless and the nurses would only tell me “they won’t let you out while you act like this”. When I couldn’t sleep I told the nurse watching me that I couldn’t sleep and all she said was “you slept”. So I got a coffee at 4am and waited for the day to pass. When your days start at 4am and you don’t get to go to bed until 9pm the days are pretty long and shitty. I’d been managing to quit smoking but when I got in there it was the only thing that allowed me to go outside for 5 minutes.
I was too anxious to shower with someone watching me and I was told me not showering would go against me and I would be made to stay longer. On one particular night they gave me Lorazepam, Zopiclone and Quetiapine all in one night and it made me hallucinate. My birth/dead name was used quite frequently until my named nurse took notice, however that didn’t stop some of the nurses from being ignorant. I was found crying by a nurse who had been extremely harsh and blunt with me from the start of my time there, she gave me no sympathy or advice, just another broken record “do you really think they’ll let you out while you’re acting like this?”. I was saddened to hear that it would go against me to portray my emotions.
I made friends on the ward, they were very good people and I still contact them to this day, I’ll always be grateful for them. One occasion that stood out to me was when I was taken into the office and told “some patients” were “unhappy” with me being on the male bedroom corridor, I was given a rape alarm but wasn’t told who would potentially be attacking me. I was offered food but was too anxious to eat in front of the other patients, the nurses refused to let me eat alone and I had to sit in between two armchairs in the corner. I declined food for the first 3 days and lost weight drastically, I was malnourished, dehydrated and tired, but yet again I was told this was all going against me. I wasn’t offered any advice. A nurse came to me asking about what I wanted to eat, asked me if I wanted a vegan meal and I accepted, she then looked at the list of things and replied “oh well, we don’t have any” and I was forced to choose something else. I was even given meat at one point that I refused to eat.
On my last night I was kept up until nearly midnight because they were late doing night medications (meant to be given at 9pm), my friend and I were the last two to get ours. My review session was 5 days after I was sectioned, I was in the room for 15 minuets, lied through my teeth about feeling great and not wanting to die; I was let out immediately after. They told me I was going to be kept inside this place for all the times I fucked up that I couldn’t help because I was mentally ill. Then I was let out within 15 minutes of lying.