This Page in kept Updated HERE

This Page in kept Updated HERE
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RITB are delighted to be able to share a recent keynote delivered by Raza Griffiths (above), lead author of the Kindred Minds Manifesto. Here’s what Raza said about the keynote:

I used the powerpoint as part of my opening keynote at a conference entitled “Psychological impacts of racial discrimination for both clients and practitioners”. The event was organised by practitioners from the British Psychological Society – which, as a professional body, has had a patchy history when it comes to addressing racism.
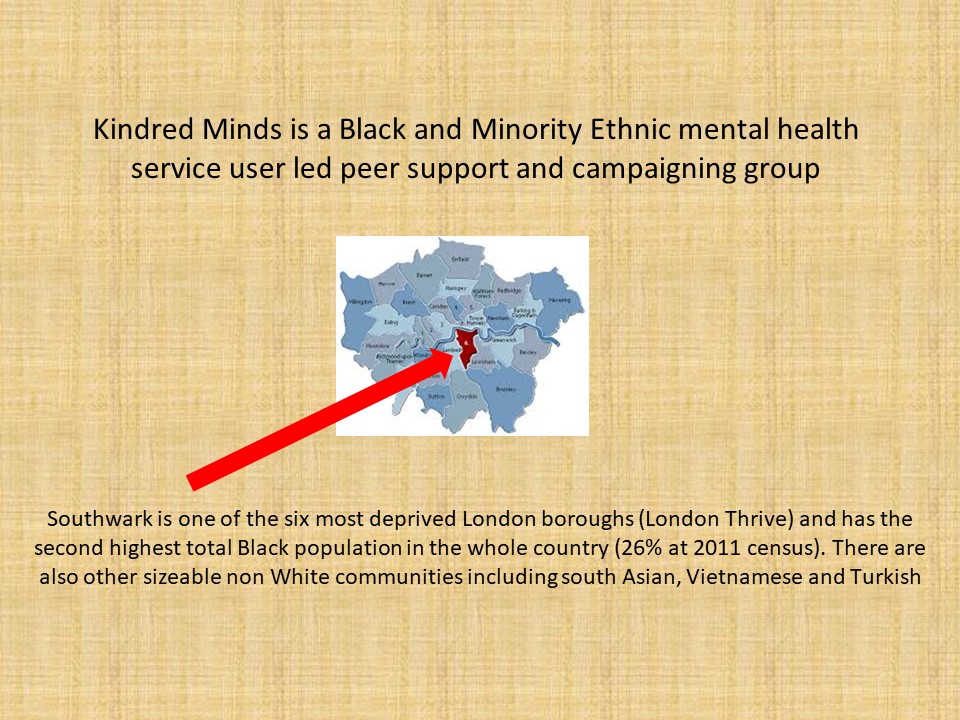
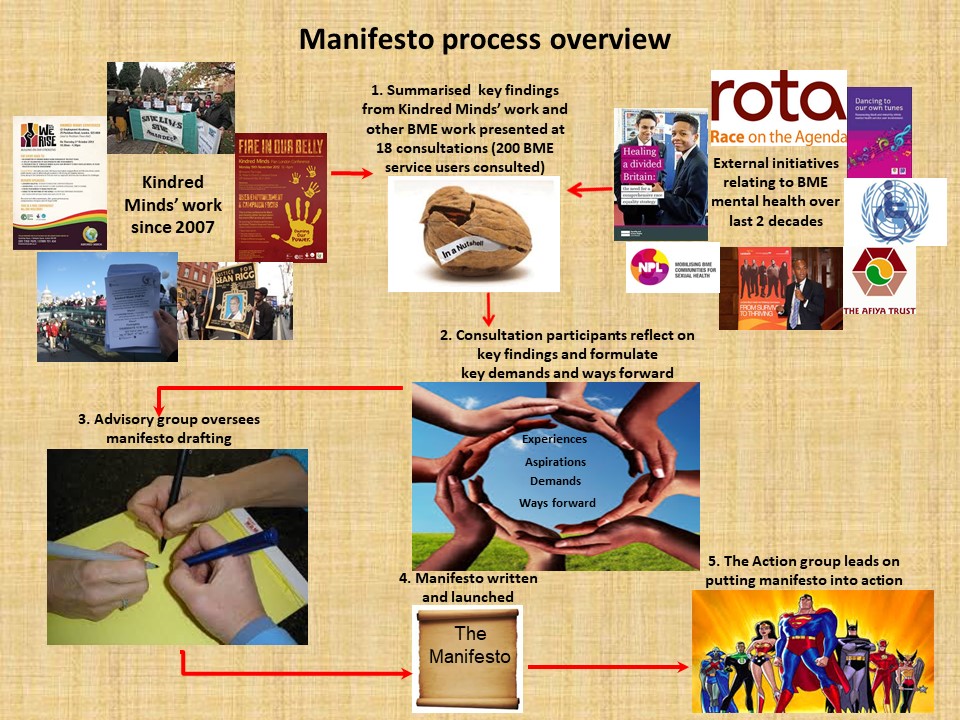
For this event, I looked primarily at the impact of racism on BME service users, drawing on my work in authoring “A Call for Social Justice” (2018). This is a manifesto written with contributions from 200 BME mental health service users, and spells out the changes they have said are needed to bring about a reduction in BME communities’ poor experiences within ‘mental health’.
The manifesto underlines the need for action against structural and institutionalised racism. It gives an overview of the current political climate and then identifies the changes in policy and practice across a range of interlinked life areas, including in education, policing and mental health, that BME service users have said will bring about an improvement in their mental wellbeing.
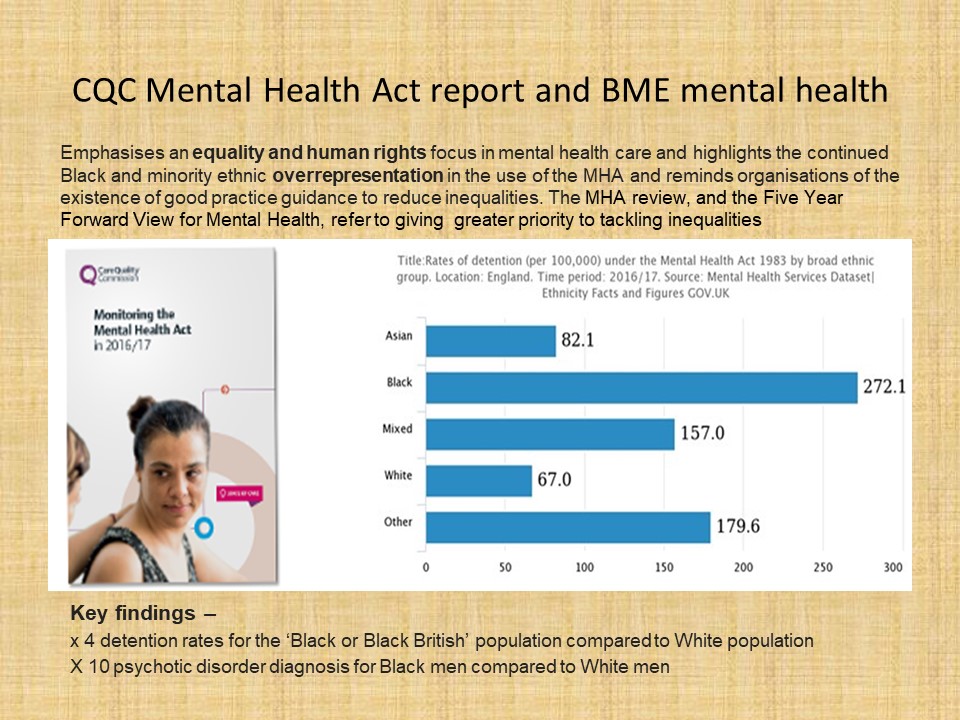
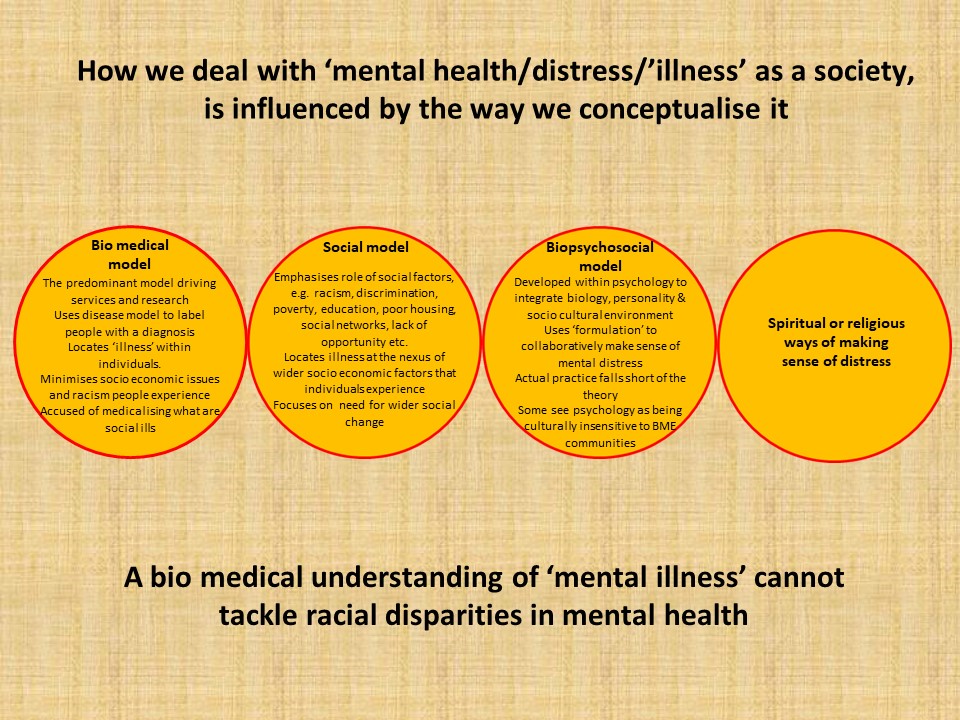
In mental health, this includes a move away from an exclusive focus on bio medical understandings of mental distress and towards support underpinned by a plurality of understandings of distress that BME communities can relate to; a move away from involuntary detention and treatment which are disproportionately used against BME communities; and foregrounding some of the good practice identified by the extensive writings of BME service user led initiatives over the years which are all too often ignored by campaigning groups and policy makers.
The conference took place on Friday 11th October 2019 at the De Vere Grand Connaught Rooms in Holborn, London
Links to the executive summary and full version of the manifesto can be found at the bottom of this webpage: https://www.nsun.org.uk/news/bme-mental-health-service-users-launch-manifesto



















DISCLAIMER: RITB holds a neutral position on medication – we support people to make their own freely informed decisions based on their preferences and circumstances – this includes taking medication and also includes not taking medication (and anything in between!). RITB has produced a position statement on Borderline Personality Disorder (BPD), which we encourage everyone to read. RITB has used publicly available information to compile this blog.
CONTENT WARNING: This blog describes the serious and potentially fatal side-effects and risks associated with clozapine.
Update: 23.10.19: RiTB has recieved confirmation from the Health Research Authority (HRA) that they are investigating the concerns raised in this blog. You can contact the HRA and Trial Sponsor yourself: HRA: hra.complaints@nhs.net Sponsor (Imperial College): jrco@ic.ac.uk
We published a follow up blog documenting the complaints and concerns process on the 16.12.2019, which you can find HERE.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
There’s been a lot of twitter noise recently about the CALMED Trial – a Randomised Controlled Trial (RCT) of Clozapine for people diagnosed with Borderline Personality Disorder (BPD). 111 people will receive clozapine and 111 will receive a placebo for 6 months. A number of concerns have been raised online about this trial, particularly by service users. This blog will focus primarily on the trial population (the people invited to take part in the study) and associated ethical concerns, particularly in relation to the risk vs benefit principle.

To understand the risk vs benefits involved with this trial, we must start with an introduction to clozapine – the medication being prescribed….
Clozapine is an antipsychotic licenced for people who have been diagnosed with ‘treatment resistant’ schizophrenia, and you can read more about it here. Clozapine is associated with severe and fatal side effects. The FDA have issued 4 black box warnings (the UK and EU do not have an equivalent system) in relation to Clozapine for those under 65, which include:-
Black box warnings are reserved for medications with severe and life-threatening side-effects. Antidepressants typically have 1 black box warning, which pertains to increased suicidality in children, adolescents and younger people. Clozapine’s black box warnings are echoed in the BNF (the UK medication bible), which also highlights an additional potentially fatal side-effect:-
Given clozapine’s potentially fatal nature, it requires extensive routine monitoring, particularly in the first 6 months (when most severe adverse effects are likely to occur), which includes: –
All people taking clozapine in the UK must be registered with one of three authorised clozapine monitoring services, one of which includes the Clozaril Patient Monitoring Service (CPMS). A satisfactory blood result must be approved by a monitoring service before another prescription is issued. For the first 18 weeks this prescription is typically weekly, after 18 weeks fortnightly, and after a year monthly. Patients must collect prescriptions from a designated clozapine dispenser in their locality, which is typically not their local pharmacist.
No other medication used to treat mental health conditions in the UK requires such extensive monitoring and infrastructure. Agomelatine (an atypical antidepressant) and some mood stabilitsers including lithium and carbamazepine require on-going monitoring, but this is not as frequent, and they don’t require a national monitoring infrastructure.
In addition to extensive monitoring and potentially fatal side-effects, clozapine has also been associated with other significant side-effects, including rapid and substantial weight gain, sedation and sialorrhea (excessive saliva pooling especially at night). Long-term side effects include diabetes and cardiovascular diseases. These side-effects are more severe compared to medications like antidepressants and compared to other antipsychotics. Caution must also be taken when stopping clozapine: the BNF recommends a 1-2 week withdrawal period and like all antipsychotics it is associated with a high risk of relapse after long-term use on discontinuation.
To sum up – Clozapine is in a class of its own when we look at medication in the mental health world. No other drug has this many black box warnings, monitoring requirements and significant side effects. It is a special case.
As a special case, clozapine prescriptions are typically limited to people diagnosed with ‘treatment resistant’ schizophrenia, who have tried at least 2 other antipsychotics, one 1st generation and one 2nd generation (the generations aren’t too important here). Some studies indicate that for people with this diagnosis, clozapine reduces suicide rates (this is disputed by others); and is more effective than other antipsychotics on outcomes including relapse rates and hospitalisaiton. In clinical practice, prescribing clozapine for ‘treatment resistant’ schizophrenia is still a short and long term risk vs benefit balancing act: if it does reduce suicide rates, relapse and hospitalisation, short and long term side-effects may still be fatal.
Let’s move now to Borderline Personality Disorder (BPD). It’s important to note that BPD is a highly contested diagnosis, probably more so than any other mental health diagnosis, and for good reason. Unfortunately, this blog cannot do justice to the plethora of concerns about this diagnosis, but you can read more about them here and you can read RITB’s position statement on BPD here.
For the purposes of context setting, the NHS website states that:
“Borderline personality disorder (BPD) can cause a wide range of symptoms, which can be broadly grouped into 4 main areas. The 4 areas are:
Psychosocial interventions are considered the most successful and clinically appropriate interventions for people diagnosed with BPD. Reflecting this, NICE guidelines state that medication (any mental health medication) should:
“not be used specifically for borderline personality disorder or for the individual symptoms or behaviour associated with the disorder (for example, repeated self-harm, marked emotional instability, risk-taking behaviour and transient psychotic symptoms).”
NICE specifically emphasise that antipsychotic drugs (clozapine is an antipsychotic):
“should not be used for the medium- and long-term treatment of borderline personality disorder.”
During a crisis, NICE asserts that short-term use of medication “may be helpful”. However this statement comes with a number of caveats, including: avoiding polypharmacy; using the minimum effective dose; ensuring that a drug is not used in place of other more appropriate interventions; and arrangements for discontinuing medication after short-term use.
Whilst NICE guidelines state that medication shouldn’t normally be prescribed for BPD, many people with this diagnosis are prescribed medication, typically antidepressants, mood stabilisers or anti-psychotics. It is widely acknowledged that clozapine is prescribed off-label for people diagnosed with severe BPD, who are typically in long-term specialist or secure units. This is supported by ‘low quality’ evidence, including a case series of 22 women with a diagnosis of BPD in a secure unit and a qualitative study on the experiences of 20 women in secure care who have a diagnosis of BPD.
To date, ‘low quality’ research investigating clozapine for people with a diagnosis of BPD primarily derives from a specific ‘sub-population’ – those diagnosed with severe BPD who are inpatients, typically in long-term secure units. This ‘low quality’ evidence, coupled with routine off-label prescribing for this ‘sub-population‘, was used by the NIHR to justify their 2016 commissioning brief for a RCT to investigate the effectiveness of clozapine for BPD. They outlined that the following ‘problem’ should be addressed by the trial:
“A significant proportion of psychiatric inpatients in secure hospitals meet the diagnostic criteria for borderline personality disorder (BPD)…..even though there are no drugs licensed in the UK for the treatment of BPD, and despite guidance, many patients are treated largely or entirely with medication. This routine practice of prescribing psychotropic medication to manage personality disorders has recently been confirmed in UK secure psychiatric hospitals where it was found that clozapine is the antipsychotic of choice for a significant proportion of inpatients with BPD.”
In response to the NIHR commissioning brief, the CALMED Trial was funded. Its study protocol (a large document that tells you everything about a study) references the same ‘low quality’ evidence and routine off-label clinical practice in its introduction. In addition to the two studies described, which involved inpatients diagnosed with severe BPD in long-term secure units, it references an evidence review conducted by Beri and Boydell (2014). This review found 12 ‘low quality’ studies (no RCT’s), 6 of which involved people with a diagnosis of BPD who also had psychosis (psychosis is most frequently experienced by people who have a diagnosis of schizophrenia, but can be a diagnosis in itself and can be a symptom of severe BPD and Bipolar Disorder). Of the remaining 6 studies: 2 were conducted in secure units, and 4 consisted of case reports, reporting on a total of 7 inpatients, who had a diagnosis of severe BPD and had not responded to a plethora of psychosocial and pharmacological interventions. For these individuals, clozapine was used as a last resort.
BUT (and this is a big BUT), the CALMED trial is not limiting recruitment to this specific ‘sub-population’ of people diagnosed with BPD (see trial protocol inclusion / exclusion criteria):
People with a diagnosis of mild, moderate and severe BPD, who are admitted to non-secure, short-term mental health wards, including general acute wards, are currently being invited to take part in this trial in multiple NHS Trusts. All publicly available information about the study confirms this, including (but not limited to): the study protocol, a recent presentation at the 2019 Royal College of Psychiatrists Forensic Faculty Conference and reports from people using services on social media.
However, a RCT has not yet demonstrated that clozapine is effective for the original ‘sub-population’ for whom the trial was deemed necessary by the NIHR (based on available ‘low quality’ evidence and off-label prescrubing practices): people who have a diagnosis of severe BPD, who have not responded to all other evidence-based interventions, and who are typically long-term inpatients in secure units.
Perhaps of most concern is that the CALMED Trial is not using clozapine as a last resort intervention. Inclusion and exclusion criteria do not ensure that participants (whatever their setting or BPD severity) have been offered and have declined, or have failed to benefit from, NICE recommended individual and group psychological therapies. Neither do they ensure other NICE recommended assessments or interventions are provided or offered to those known to have experienced trauma (frequently associated with a diagnosis of BPD).
Furthermore, lower thresholds are being used for inclusion in the CALMED Trial than what NICE and the BNF recommend when prescribing clozapine for ‘treatment resistant’ schizophrenia (at least 2 antipsychotics have failed). The CALMED Trial requires only 1 antipsychotic to have been tried for at least 3 months, and the trial protocol does not justify this lowered threshold. This is significant, particularly when examining studies comparing the effectiveness of clozapine to other antipsychotics for people diagnosed with ‘treatment resistant’ schizophrenia. Studies using higher thresholds to define ‘treatment resistant’ report larger effect sizes compared to with those that fail to define ‘treatment resistance’ (some of which report no difference in overall effectiveness).
It is unclear why the CALMED Trial is not limiting recruitment to people who have a diagnosis of severe BPD, who have not responded to all other evidence-based interventions, and who are typically long-term inpatients in secure units. Diversions from the original NIHR commissioning brief’s ‘problem’, ‘low quality’ evidence, and off-label clinical practice are not justified in the study protocol. However, the NIHR highlighted in their commissioning brief that…
“The setting, whilst challenging for recruitment, would allow close monitoring of any adverse effects”.
It is unclear what “setting” the NIHR were referring to, however, this statement follows a paragraph (quoted above) which makes multiple references to secure inpatient settings only.
Secure settings may indeed be challenging for recruitment. However, such challenges do not render it ethically justifiable to expose a different vulnerable population to a medication that poses multiple monitoring burdens and potentially fatal risks. For this population, NICE clinical guidelines recommend no medications, standard clinical practice does not constitute the off-label prescribing of clozapine, and psychosocial interventions are the first line treatment. The CALMED Trial’s inclusion and exclusion criteria significantly diverges from standard clinical practice for this population and the existing evidence base.
The 2016 NIHR commissioning brief outlined that the “setting” (which we can only assume refers to secure units) “would allow close monitoring of any adverse effects”. However, by broadening the population eligible for this trial, the “setting” and the safeguards relied on by the NIHR have diminished. Staffing numbers on general acute mental health wards are significantly less than those in secure units, and people do not typically stay long-term on acute mental health wards, with pressures to discharge increasing continuously.
It is important to acknowledge that clozapine is often initiated on general acute mental health wards for people diagnosed with ‘treatment resistant’ schizophrenia. However, this is congruent with standard clinical practice and clozapine licencing. Risk vs benefits thresholds are higher for clinical trials, particularly for a population for whom clozapine is not being used as a last resort and who may not have received NICE recommended therapies.
The trial’s initial publicly available protocol (Version 2.0) specified that people who were due to be discharged within 2 weeks would be excluded from participating. This meant that you had to be an inpatient for at least 2 weeks after starting the trial. On the 21.8.2019 exclusion criteria were amended to enable people to take part as an outpatient if they are due to be discharged within 2 weeks, with a caveat about monitoring in the community.
The original safeguards anticipated by the NIHR’s commissioning brief, associated with secure long-term inpatient ‘settings’, have been further eroded. The most serious adverse and fatal side-effects often occur within the first few weeks and months of taking clozapine. Clozapine requires extensive monitoring up to 18 weeks and then indefinitely. This doesn’t just include bloods – it includes monitoring to ensure constipation is treated quickly and to respond to signs of infection or cardiac problems, all of which can be fatal.
Someone who has a diagnosis of BPD, who is acutely unwell and in crisis frequently, may not be able to manage this extensive monitoring in the community for a drug they would not normally be prescribed, contrary to best practice guidelines. Who will monitor these participants in the community at a time when community resources are already stretched too far? The most recent publicly available trial protocol (Version 3.0) does not outline what additional measures are being put in place to manage these increased risks in a community setting.
Whilst there are ethical issues relating to the ability of people in secure settings to provide free and informed consent to a trial (e.g court orders and the MHA), similar issues pertain to those on general acute wards. People using services have recently spoken openly on twitter about their experiences of being approached to participate in this study, which have been deeply distressing.
We cannot examine all potential factors that could limit freely given informed consent here. But, it’s important to note that people with a diagnosis of BPD are often considered the most stigmatised and poorly treated patients by mental health professionals. They are frequently not provided with NICE recommended psycho-social interventions in the community or as inpatients, and may be desperate for any potential intervention to alleviate their suffering.
Participant Information Sheets (PIS) (a long document that tells people everything about the study) are essential in ensuring consent to any research is informed. Like most studies, the CALMED Trial’s patient information sheets are not publicly available online (at the time of publication: PIS have been requested from the study team but have not been received). Therefore, it is not possible to determine if the CALMED Trial’s PIS ensures that participants will be informed about clozapine’s significant risk profile and about the trial’s diversions from standard clinical practice and existing ‘low quality’ evidence. Information publicly available for potential participants on the ‘Be Part of Research’ website states:
“As with any medicine, side effects are possible with clozapine, however, not everyone who takes the medication will experience problems”
This severely underplays the reality.
All people conducting clinical research in the UK must adhere to The Declaration of Helsinki (2013) (a set of ethical principles used across the world for research involving human subjects). The Declaration is intended to be read and understood in its entirety, however, for the purposes of understanding the CALMED Trial’s tipping point, it states that:
“Medical research involving human subjects may only be conducted if the importance of the objective outweighs the risks and burdens to the research participants.”
This principle has a higher threshold for ‘vulnerable groups and individuals’ who receive “specially considered protection” under the Declaration. People diagnosed with BPD who are currently inpatients or outpatients – in whatever mental health setting meet this criteria. As such, they:
“…should stand to benefit from the knowledge, practices or interventions that result from the research.”
Whilst it could be argued that clozapine prescribing as a last resort may benefit people who have been diagnosed with severe BPD, typically in long-term secure settings (based on ‘low quality’ research and off-label prescribing practices), this does not extend to others diagnosed with BPD.
The Declaration also has a specific section on the “Use of Placebo”, which the CALMED Trial is comparing to clozapine. It’s worth reading this section in full:
“The benefits, risks, burdens and effectiveness of a new intervention must be tested against those of the best proven intervention(s)….
The best proven intervention(s) for BPD, as recommended by NICE, are long-term psychosocial individual and group interventions. These are not being compared to clozapine in the CALMED Trial. However, the declaration offers 3 exceptions:
1.“Where no proven intervention exists, the use of placebo, or no intervention, is acceptable”
As outlined, proven interventions exist and the CALMED Trial is not using failure to respond to, or accept, recommended psychosocial interventions as an inclusion / exclusion criteria.
2.“Where for compelling and scientifically sound methodological reasons the use of any intervention less effective than the best proven one, the use of placebo, or no intervention, is necessary to determine the efficacy or safety of an intervention”
The CALMED Trial protocol does not provide compelling and scientifically sound methodological reasons for conducting a trial in a population for which it was not intended, and for which clozapine is not supported by existing evidence, best practice guidelines, and current practice.
3. “…patients who receive any intervention less effective than the best proven one, placebo, or no intervention will not be subject to additional risks of serious or irreversible harm as a result of not receiving the best proven intervention. Extreme care must be taken to avoid abuse of this option.”
This criteria cannot be met for participants who are not receiving clozapine as a last resort intervention.
In the quest for ‘robust’ evidence, and what appears like attempts to overcome recruitment challenges, the CALMED Trial is conducting a RCT in a population for whom the trial was never intended. Clozapine is not being used as a last resort intervention, it is not being prescribed in accordance with best practice clinical guidelines for both BPD and ‘treatment resistant schizophrenia’, nor in accordance with existing ‘low quality’ evidence. It therefore places vulnerable people who would never normally be prescribed clozapine at risk in the quest to generate knowledge for a very different population. Hierarchies of evidence are not ethically neutral or without bias. The gold (standard) does not always glisten.
Conflict of Interest Statement: RITB’s financial disclosure can be found here. RITB has never and will never receive funding from any pharmaceutical company. RITB is not affiliated with any academic institution or pharmaceutical company.

Amendments: 18:54 on the 22.10.19 – The article originally stated that all people prescribed clozapine must be registered with the CPMS. It now states that they must be registered with one of three authorised services, which includes the CPMS. 8:15 am on the 23.10.19 to remove a factual inaccuracy about the exclusion of people who have psychosis.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
I am furious with the mental health awareness campaign. I am seething at the lie that if we put our mentally ill heads above the parapet and reach out, we will be seen and heard and given help. I am livid about the fact that mental health seems to be the great issue of our times, yet for those of us with severe and enduring mental illnesses, cuts to vital services mean that dreams of even the most basic long term care are the reality of a bygone era.
I want to force public attention away from the well-meaning awareness campaign and towards the lack of crisis care available, towards the state of our seriously ailing social services, and towards the effects of austerity measures which have put the lives of the most vulnerable in society at the most risk.
But there is absolutely nothing I can say which hasn’t already been said. The statistics are clear and damning and public. Writers have won awards for their criticism of the mental health conversation. Yet we continue to be blasted by a message of awareness which skates over the truth in a way that puts us all at risk. So I am going to shout about the reality of the situation, of my situation, in an effort to redress the balance of the conversation we so desperately need to be having.
The reality is urgent referrals getting lost or delayed on numerous occasions. It is being in a life-threatening situation and put on hold for hours by a specialist crisis line whose voicemail message reveals that the mental health ‘team’ patients are encouraged to seek help from is in fact a single Nurse serving the entirety of South London.
The reality sees risk assessments refuse patients access to services until they are more likely than not to attempt suicide. We are pushed to the brink before we are worthy of treatment. And then there is the grand irony that we are all encouraged to reach out for help which exists only for those who can afford to pay.
I am tired. I am exhausted from living with a condition that often sees my emotional state vary from ecstatic to suicidal multiple times a day. Recently I have started to hallucinate. I am terrified of slipping back into crisis because I know that when I call for the help that I need I will not get it. I know that the more ill I become, the harder I will have to fight for my basic right to mental healthcare.
I am burdened with an unbearably cruel illness which tells me that I am wrong to write this and wrong to expect any help because I am not worth a breath of energy from anybody. And I am starting to wonder if my experiences of the system have fuelled my belief that nothing I go through could be bad enough to warrant serious and thorough treatment. This is all making me sicker.
Countless stories like these are already in the public domain. It often feels like I’m screaming into an echochamber filled with other mental health service users who too are facing year-long waits for help with conditions that are life threatening now. We have been shouting from the rooftops while well-meaning ideas of awareness and resilience are banded about like they will solve everything. Of course #EveryMindMatters. But shining a light on mental ill-health and failing to acknowledge the grossly inadequate systems which exist to deal with it often just serves to exacerbate the issue.
I don’t want you to respond with sympathy. I want you to be angry. I want you to share my outrage, the outrage I felt when I was sent away from more than one health provider, suicidal and alone, because I was not on the right list to qualify for help. I want your awareness to be centered on the situations that thousands of us face daily as we continue to keep our heads above the water while fighting a battle that should not exist.
The chances are that you’ve already read something like this. My experience is not unique. Please, if you are mentally healthy, take my anger and do something productive with it, because I have run out of energy and this crisis is growing. Please share the fight with me.

